While athletes work hard to keep their bodies in top condition, it's important to take time to relax. People relax by enjoying alcohol with friends or just a casual drink. The amount of alcohol consumed and the tolerance of each individual will determine how it affects them. A few drinks can ruin your hard work, erase the benefits of your workouts, reduce your endurance and compromise your mental fortitude. Keep track of how many drinks you have and how you feel the next day to determine your tolerance.
ALCOHOL'S EFFECTS ON MUSCLE RECOVERY AND DEVELOPMENT
Muscle health is key to athletic success. Science has shown that alcohol can cause muscle damage and even rob you of all your weight training. Here's why:
Impairs muscle growth
Exercise under the influence can increase your risk of injury and cause muscle loss. The effects of long-term alcohol consumption on protein synthesis can lead to a decline in muscle growth. Even short-term alcohol use can affect your muscles.
Dehydrates your body
You want to maximize your athletic performance by speeding up your recovery from sore muscles. This is due to the fact that alcohol can be a diuretic and cause electrolyte imbalances and dehydration. Dehydrated athletes are more susceptible to cramps, muscle pulls and muscle strains.
Prevents muscle recovery
To build bigger muscles, it is important to get enough sleep. Drinking alcohol can adversely affect your sleep patterns and cause your body to lose a chemical called HGH (human growth hormone). Although HGH is essential for building bigger muscles, alcohol can reduce HGH secretion by up to 70%. Also, binge drinking can lower serum testosterone levels. A decrease in testosterone can lead to a decrease in muscle mass and recovery. This can cause performance problems.
Depletes your energy
Your body's water balance can be disrupted when alcohol is absorbed via your small intestine, stomach, and into your cells. An imbalance in water levels in muscle cells can cause them to stop producing adenosine triphosphate (ATP). This is an essential fuel for all cells including our muscles. A decrease in your body's ATP levels can lead to a loss of energy and endurance.
Slower reaction time
Even small amounts of alcohol can cause a slower reaction time and impaired hand-eye coordination. This can not only affect performance but can also increase your chance of injury.
NUTRITIONAL EFFECTS OF ALCOHOL
It cannot be used to produce energy.
Our tendency is to believe that only carbohydrates, proteins, and fat can provide energy in the form of calories. This is not an exhaustive list. Alcohol has 7 calories per Gram (roughly halfway between the calorie values of carbs or fat). Your muscles cannot use alcohol calories as fuel, unlike the calories we get from food. Your body does not convert alcohol calories to glycogen, which is a form of stored carbohydrates. They are therefore not a good source for energy during exercise. Instead, your body converts alcohol energy into fatty acids and stores them within our fat tissue. Alcohol consumption can increase fat storage, which can negatively impact your body's percentage of fat.
It prevents nutrients from being absorbed.
The nutritional value of alcohol is very limited because it is devoid of vitamins and minerals. It also prevents your body from receiving these nutrients from other sources.
Thiamine (vitaminB1): Thiamine plays a role in the metabolism of food into fuel and the formation of hemoglobin. Vitamin B1 is vital for optimal performance because it plays a part in the metabolism of carbohydrates.
Vitamin B12: Vitamin B12 is essential for maintaining healthy nerve cells and red blood cells. Anemia is a condition where alcohol can prevent b12 from being used by your body in key processes.
Folate: Folic Acid is part of a coenzyme that helps in the formation red blood cells. Folic acid deficiency can lead to a lower VO2max which can adversely affect your endurance.
Zinc: Zinc is an essential component of energy metabolism. Your body's zinc resources can be depleted by alcohol, which can lead to a decrease in endurance.
EXERCISE AFTER A HANGOVER
Hangovers can be caused by alcohol toxicity, dehydration and toxic effects of congeners, which are found in many alcoholic beverages. You've likely experienced the symptoms of nausea and soreness, depression, headaches, and a promise to stop drinking alcohol again if you have ever had a hangover. These symptoms can cause a decrease in athletic performance, and even a 11% reduction in aerobic performance. If you feel nauseous, you should not exercise. It can increase your chances of injury and dehydrate you further.
As alcohol affects the hand-eye coordination, imagine yourself playing cricket and misjudging how far you are from the ball. You will find it difficult to make quick decisions on the court or field because of your inability to think clearly. This could lead to devastating consequences for you and your team. You are more likely to get cramps, pulls, and strains if you drink alcohol, regardless of what sport or activity it is. It is important to remember that alcohol can impact bone growth and make it more difficult to repair bone damage if you are injured. Your career can be affected.
A
Ask your doubts
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
Related Blogs
read count
read time
Hormone Health
Jun 10, 2026
Did You Know Poor Sleep Can Trigger Weight Gain Hormones Overnight
We live in a world that glorifies hustle culture - late nights, early mornings, and the belief that sleep is a luxury. But what if those lost hours of rest are quietly working against your weight loss goals?
Introduction
Many people believe weight gain happens slowly through diet or inactivity. While these factors certainly influence body weight, an often overlooked driver of metabolic imbalance is poor sleep.
Sleep is not simply a period of rest. During the night, the body performs critical metabolic repairs that regulate hunger hormones, insulin sensitivity, and energy balance. When sleep quality becomes disrupted, these biological processes can change within a single night.
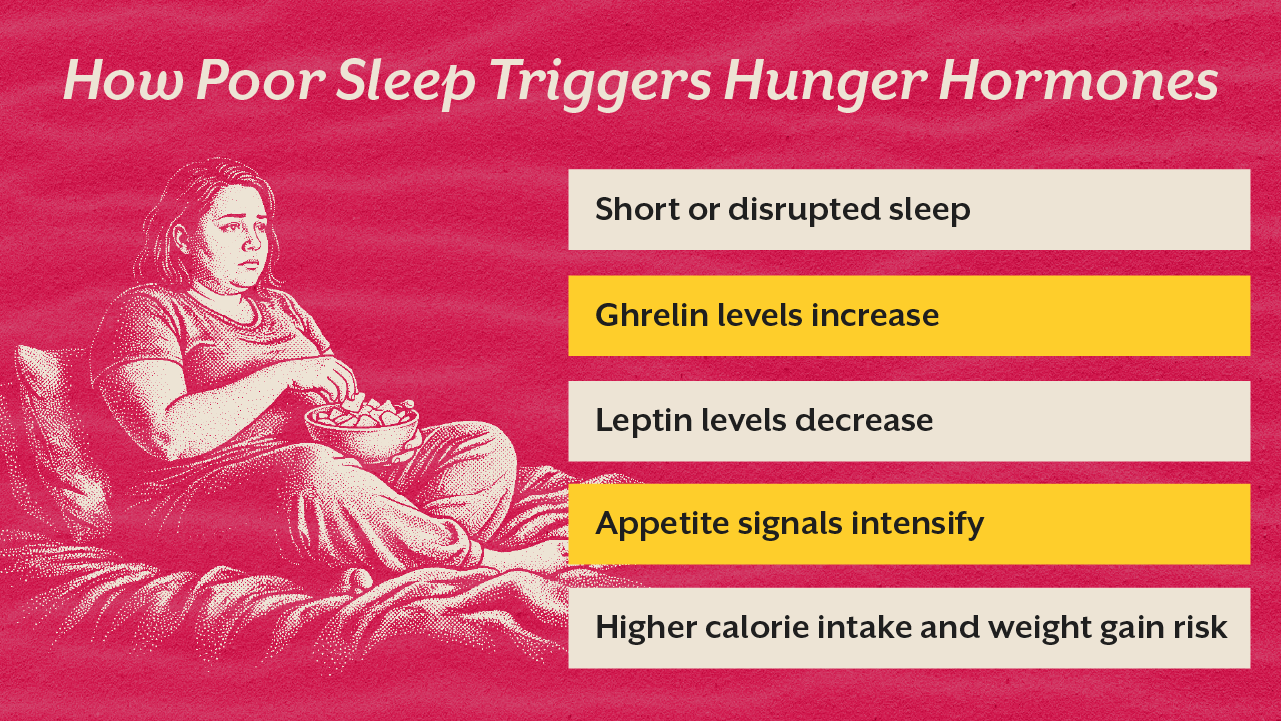
Studies on sleep deprivation and weight gain show that even short periods of poor sleep can alter appetite hormones such as ghrelin and leptin. Ghrelin stimulates hunger while leptin signals satiety. When sleep becomes fragmented or shortened, ghrelin levels rise while leptin declines. This imbalance often increases cravings for high calorie foods the following day.
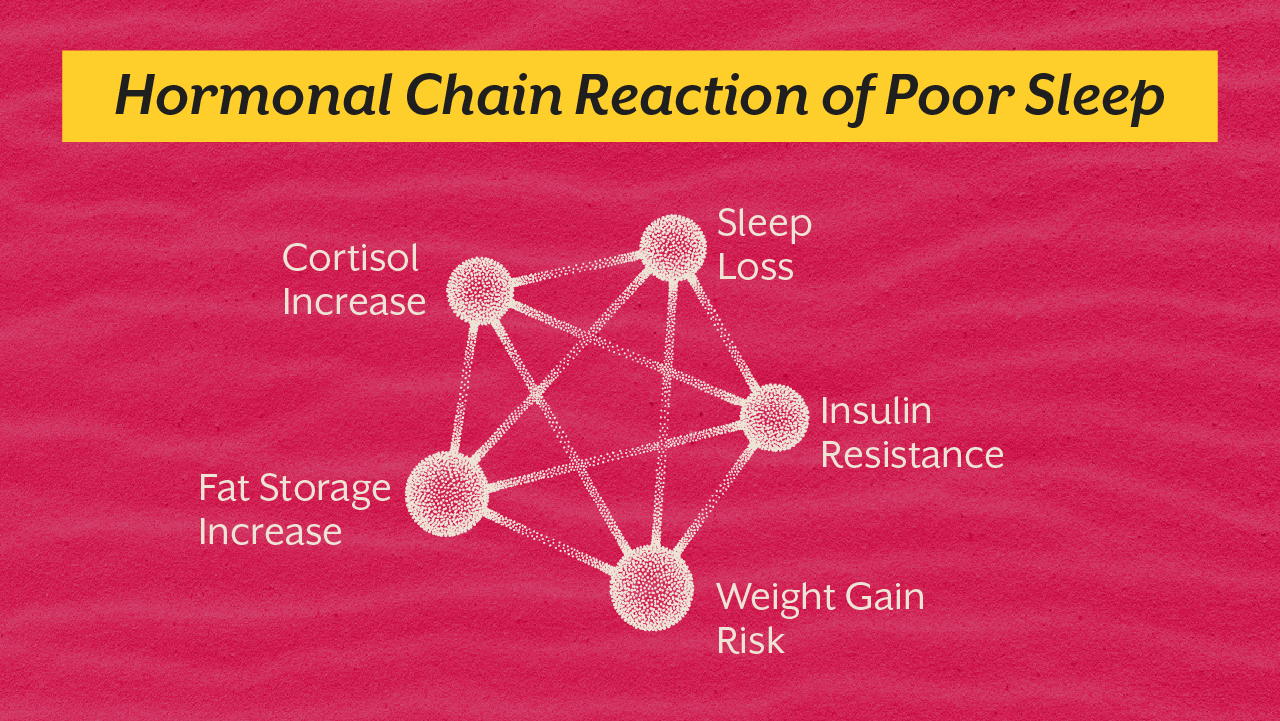
Beyond hunger signals, poor sleep hormones and weight gain pathways involve deeper metabolic changes. Cortisol levels increase when the body perceives stress or sleep loss. Elevated cortisol encourages fat storage, particularly around the abdomen.
At the cellular level, mitochondrial function also plays a critical role. Mitochondria regulate energy production and metabolic signaling. When sleep becomes inconsistent, mitochondrial efficiency declines, reducing the body’s ability to perform overnight metabolic repair.
At iThrive Alive we often see individuals struggling with stubborn weight gain despite healthy diets. In many cases the underlying driver is not just food choices but disrupted sleep biology. Understanding how sleep and weight gain interact can help individuals fix sleep to lose weight naturally rather than relying only on restrictive dieting.
The Overnight Metabolic Reset That Happens During Sleep
Why Sleep Is Critical for Metabolic Repair
Sleep is a metabolically active state. While the body appears still, several hormonal and cellular systems become highly active.
Growth hormone release increases during deep sleep and supports fat metabolism. The brain also regulates appetite hormones that influence hunger the next day. At the same time mitochondria repair cellular damage accumulated during daily metabolic activity.
When sleep duration falls below optimal levels these processes become impaired. The body may wake up in a metabolic state that favors hunger signals, insulin resistance, and fat storage.
Research summarized in the white paper “Mitochondrial Dysfunction Sleep Deprivation Sleep Disorders” highlights how disrupted sleep reduces mitochondrial energy efficiency. Lower energy production can alter glucose metabolism and increase the risk of weight gain.
How Sleep Deprivation Alters Hunger Hormones
Ghrelin and Leptin Imbalance
The Hunger Hormone Shift
Ghrelin is often referred to as the hunger hormone because it stimulates appetite and food seeking behavior. Leptin performs the opposite function by signaling fullness to the brain.
Even one night of poor sleep can alter the balance between these hormones. Research shows that sleep deprivation and weight gain are closely linked through this hormonal disruption.
When sleep becomes insufficient ghrelin levels increase significantly. At the same time leptin levels decline, reducing the body’s ability to recognize satiety.
The Behavioral Consequences
This hormonal shift often results in increased cravings for calorie dense foods the next day. Many individuals notice stronger cravings for sugar and processed carbohydrates following poor sleep.
These cravings are not simply psychological. They reflect genuine biological changes in appetite regulation.
Sleep loss activates the body’s stress response. When sleep becomes fragmented or insufficient, the hypothalamic pituitary adrenal axis increases cortisol production.
Cortisol prepares the body for alertness and energy mobilization. However, chronically elevated cortisol encourages fat storage and increases blood sugar levels.
Individuals experiencing insomnia and weight gain often show elevated cortisol patterns particularly during the evening hours when cortisol should normally decline.
Metabolic Consequences
High cortisol can also impair insulin sensitivity. When cells become less responsive to insulin signals, glucose remains elevated in the bloodstream.
This metabolic state encourages fat storage and increases the risk of insulin resistance and poor sleep cycles.
Mitochondrial Dysfunction and Overnight Metabolic Repair
Why Cellular Energy Matters for Weight Regulation
Weight regulation depends heavily on mitochondrial function. Mitochondria determine how efficiently the body converts nutrients into energy.
During sleep these cellular structures perform essential repair processes. Damaged mitochondrial components are replaced and oxidative stress is reduced.
When sleep becomes disrupted this repair process becomes incomplete.
Reduced Metabolic Efficiency
Impaired mitochondria produce less cellular energy. As energy production declines the body may rely more heavily on glucose metabolism and store excess energy as fat.
This is one reason individuals experiencing sleep deprivation and weight gain often struggle to lose weight despite dietary changes.
Supporting Mitochondrial Recovery
Lifestyle interventions such as consistent sleep timing, stress regulation, and nutrient support can improve mitochondrial resilience.
Magnesium for sleep and weight loss support is often discussed because magnesium contributes to both nervous system relaxation and cellular energy production.
Key Takeaway
Sleep is far more than a nightly pause in activity. It is a biological window during which the body recalibrates hormones that control hunger, metabolism, and energy balance. Even a single night of disrupted sleep can alter ghrelin and leptin levels, increase cortisol production, and impair mitochondrial repair processes. Over time these changes create a metabolic environment that favors weight gain despite conscious efforts to maintain healthy eating habits. Addressing sleep quality is therefore a critical component of long term metabolic health. By restoring circadian rhythm, supporting mitochondrial function, and stabilizing hormonal signaling, individuals can rebuild the biological conditions necessary for sustainable weight regulation and overall wellbeing.
PCOS Renamed PMOS: Why This Changes Everything You Thought You Knew
PCOS is now PMOS, a shift that changes how we understand this condition entirely. This blog breaks down what PMOS really means, why it matters, and how looking beyond symptoms can help you address the root cause effectively.
Introduction
You literally did everything you were always told. Tried eating clean, did strength training, fixed sleep schedule and yet after all of this, something always felt off.
Your periods were still irregular, energy dipped rapidly, weight didn’t respond the way it was supposed to and somewhere along the way, you were constantly told you might have PCOS. But even that diagnosis didn’t entirely explain what you were experiencing because deep down, it never felt like it was just about your ovaries. And now finally after years, for the very first time medicine is catching up with that reality.
PCOS has officially been renamed PMOS which stands for Polyendocrine Metabolic Ovarian Syndrome.
This entire shift from pcos to pmos is more than just a change in the name. For your information it’s a complete reframing of how you understand this condition. And most importantly, it is finally being validated what women have been saying for years and years.
PCOS Renamed PMOS
Why does this change even matter?
After a global consensus including around 14,000+ women and about 56 business organisations, the term PCOS was reconsidered. Because the board finally concluded stating that the name itself was misleading.
The breakthrough of PMOS is as follows:-
PMOS is referred to Polyendocrine Metabolic Ovarian Syndrome
Polyendocrine means multiple hormone systems are involved
Metabolic related to insulin resistance at the core
Ovarian redirects to the reproductive symptoms
Earlier, pcos pmos was understood largely just as an ovarian issue.
But in reality pcos and pmos are whole-body conditions. They involve factors such as metabolism, inflammation, hormones, stress, as well as gut health. This is exactly why the shift from pcos renamed pmos is so significant. It moves complete focus from symptoms to systems.
You Don’t Need Cysts to Have PCOS (or PMOS)
One of the biggest misconceptions around pmos and pcos is that you need cysts to be diagnosed but in reality you don’t.
Many women with pcos pmos:
Have clear ultrasounds
But still experience symptoms
And still meet diagnostic criteria
But always know diagnosis can still come from factors like irregular or absent cycles, elevated androgens (testosterone, DHEA-S), along with signs of insulin resistance
So if your scan was “normal” but your symptoms weren't, trust me when I say your experience is still valid and in fact worth investigating.
The “Cysts” Were Never Really the Problem
Here’s something most of you aren’t told. Those “cysts” seen in PCOS? They are not actually cysts. They are immature follicles which are the eggs that didn’t fully develop due to hormonal imbalance.
This clearly states that the ovaries are responding to a deeper issue but they are not the root cause. And this is exactly what pcos to pmos helps in clarifying.
The Real Root Causes Behind PMOS
At iThrive, we don’t ever really stop at labels like pcos and pmos. We have always known in the nutrition field for going deeper into why exactly your body is responding the way it is.
1. Insulin Resistance
This one is the big one. Somewhere between 50–70% of women with PMOS have insulin resistance at the core and most of them have no idea.
Here's what's actually happening: when your cells stop responding to insulin properly, your body compensates by producing more of it. And excess insulin directly tells your ovaries to produce more testosterone. More testosterone means disrupted ovulation, more fat storage, more cravings and suddenly you're in a loop that no amount of clean eating seems to break.
That frustrating feeling of doing everything right and seeing no results? This is usually why.
2. Chronic Low-Grade Inflammation
When I say inflammation in pcos renamed pmos, I don't mean the kind where something visibly hurts or swells. This kind is invisible. It's quiet. And it's been running in the background for years.
At a cellular level, chronic inflammation keeps your body stuck in a constant state of alert. It stimulates the cells in your ovaries to produce more androgens. It makes your insulin receptors less responsive. It raises markers like hs-CRP and IL-6 that most standard blood panels don't even bother checking.
And you would like to know the worst part? It feeds itself. Inflammation disrupts hormones, and hormonal imbalance drives more inflammation. Round and round.
The triggers are usually coming from processed foods, a compromised gut, environmental toxins, or chronic stress. Which means until inflammation is actually addressed at the root the pmos symptoms keep coming back.
3. Stress & HPA Axis Dysfunction
We've all been trained to think of stress as a mindset problem. But physiologically, stress is a hormonal event and a serious one.
Your HPA axis is your body's central stress response system. When it's chronically activated, cortisol stays elevated. Elevated cortisol destabilises blood sugar, which increases insulin demand. And your adrenal glands start pumping out androgens like DHEA-S independently of your ovaries.
This is where it gets interesting. Even if your ovarian hormones look completely normal on paper, adrenal-driven androgens can still cause acne, hair thinning, and irregular cycles. This subtype that is adrenal pmos is especially common in women with high-pressure, high-performance lifestyles. And it gets missed constantly because nobody's looking for it.
The HPA axis is the central stress response system of your body. When it is activated repeatedly, it starts affecting multiple pathways that are involved in pcos to pmos progression.
4. Gut Dysbiosis & Leaky Gut
Your gut is deeply connected to your immune system, hormones as well as metabolism.
In pmos pcos, gut dysfunction often shows up as reduced microbial diversity, increased intestinal permeability also known as leaky gut, and overgrowth of harmful bacteria. This results in something called metabolic endotoxemia wherein the bacterial toxins like LPS leak into the bloodstream.
So what do they do?
Firstly they trigger the systemic inflammation, secondly it worsens the insulin resistance and lastly it disrupts estrogen metabolism through the estobolome.
The estrobolome which is the gut bacteria that is responsible for the procession of estrogen plays a significant role in maintaining hormonal balance.
When it’s compromised even slightly, it leads to affected estrogen clearance, worsened hormonal balance, and intensified symptoms of pcos and pmos.
This is why many women with pcos renamed pmos also report:
Bloating
Constipation or irregular bowel movements
Food sensitivities
5. Nutrient Deficiencies
This is by far one of the most underestimated drivers of pcos pmos. Because most of you including our clients who came to us initially assume that if you’re eating well, you wouldn’t be deficient.
But always remember nutrient sufficiency ≠ nutrient absorption.
In pcos renamed pmos, deficiencies are extremely common due to factors such as poor gut absorption, maximised metabolic demand, chronic inflammation and stress related depletion.
Let me take you deep into the key nutrients:
Vitamin D
Vitamin D acts like a hormone, improves insulin sensitivity and also regulates the function of ovaries.
Low levels of Vitamin D are strongly linked to insulin resistance and irregular cycles.
Magnesium
Magnesium is required for around 300 enzymatic reactions, it supports glucose metabolism and also calms down the nervous system.
Deficiency can worsen to insulin resistance and stress response.
Zinc
Zinc is critical for the functioning of ovaries, as it helps reduce the activity of androgen and also supports skin health.
Low zinc often shows up as hair fall as well as acne.
B Vitamins
B vitamins are essential for production of energy, it also supports hormone detox pathways and helps in regulating mood.
Inadequate levels can slow down the metabolic processes and further affect ovulation.
So basically besides a “healthy diet,” your body still needs smart supplementation.
6. Environmental Toxins
This is exactly where the modern lifestyle silently interferes with biology.
Endocrine Disrupting Chemicals (EDCs) such as:
BPA (plastics)
Phthalates (cosmetics, packaging)
Heavy metals (mercury, lead)
…can mimic or block natural hormones.
In pmos and pcos, this becomes particularly problematic because these chemicals bind to the receptors of hormones. Then they alter the pathways of signalling further disrupting the feedback loops between ovaries, brain, and metabolism.
Over time what happens is the body loses its ability to regulate hormones efficiently. Additionally, toxin exposure increases oxidative stress, burden of liver detox, and inflammation which further worsens the progression of pcos to pmos.
None of these causes exist in isolation. What you see in pcos pmos is an interconnected web of all the mentioned factors and treating just one symptom never really works. Therefore pcos renamed pmos is such a necessary shift.
PCOS PMOS is a multi-system imbalance, and not a single-organ disorder.
The 5 Functional Types of PMOS
Not all pmos pcos is the same.
Functional medicine identifies 5 types:
1. Insulin-Resistant PMOS
Most common which is majorly driven by poor blood sugar control.
2. Adrenal PMOS
Triggered by chronic stress and high cortisol.
3. Inflammatory PMOS
Linked to gut issues, food sensitivities, and toxins.
4. Post-Pill PMOS
Occurs after stopping birth control.
5. Hidden PMOS
Triggered by factors like thyroid dysfunction or nutrient deficiency.
Understanding your type changes everything about treatment.
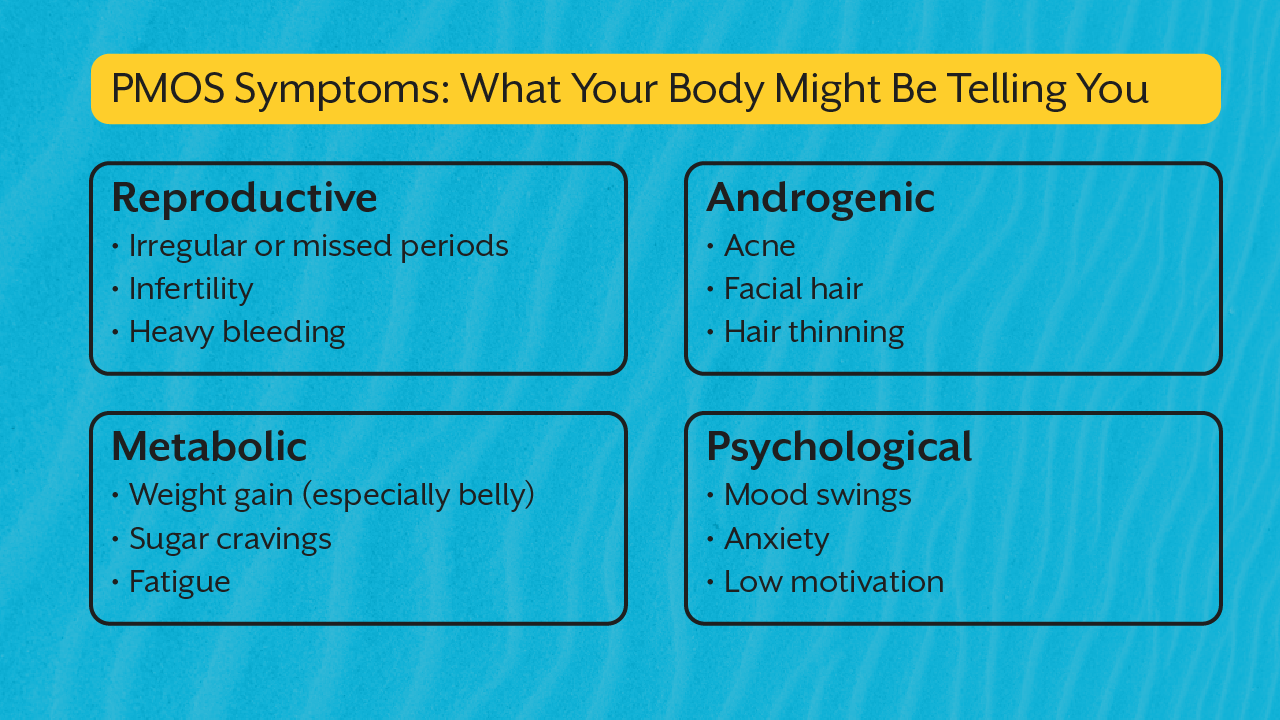
Symptoms You Shouldn’t Ignore
Pcos and pmos don't always look obvious.
It can show up as:
This is why pcos renamed needed a broader lens.
What You Should Actually Test
Instead of guessing, look deeper:
Fasting insulin
HbA1c
Testosterone & DHEA-S
LH:FSH ratio
Thyroid panel
Inflammatory markers
Book Root Cause Analysis to identify your specific triggers or if you want clarity instead of trial-and-error
Because pmos and pcos are never one-size-fits-all.
How iThrive Approaches PMOS
We have around 8 years of experience in the functional nutrition field, we’ve seen endless clients but one thing that we swear by right from the start is that we don’t just manage symptoms, we decode systems.
Our Alive Programme revolves around three factors that are personalised diet protocol, smart supplementation and lifestyle interventions. Because the goal has never been suppression it has always been reversal.
Key Takeaway
For years, most of you have been told to just lose weight, everything is normal, acne would disappear, and that this is common. But now, with pcos renamed pmos, the narrative has finally and for once changed. Because your body was never confused, it was always communicating.
Each and every symptom, the fatigue, the irregular cycle, and the sweet cravings were a signal. And now that we finally understand pcos and pmos the way it was always meant to be understood.. you’ve got a choice.
Either to ignore it again or to finally listen and book a root cause analysis to know the triggers so we start reversing as soon as possible. Because healing doesn’t begin when symptoms disappear. It begins when you start understanding what your body has been trying to tell you all along.
read count
read time
Hormone Health
Mar 24, 2026
Hyperprolactinemia: Is This Why Your Period Disappeared
High prolactin could be silently wrecking your periods, fertility, and mood. Learn the real symptoms of hyperprolactinemia in women and what to do about it.
Introduction
Picture a 28 year old woman in India. Her periods have been irregular for over a year. She has been told she probably has PCOS. Her thyroid panel came back normal. She has been put on birth control to regulate her cycle, but the moment she stops, the irregularity returns. Nobody has checked her prolactin yet.
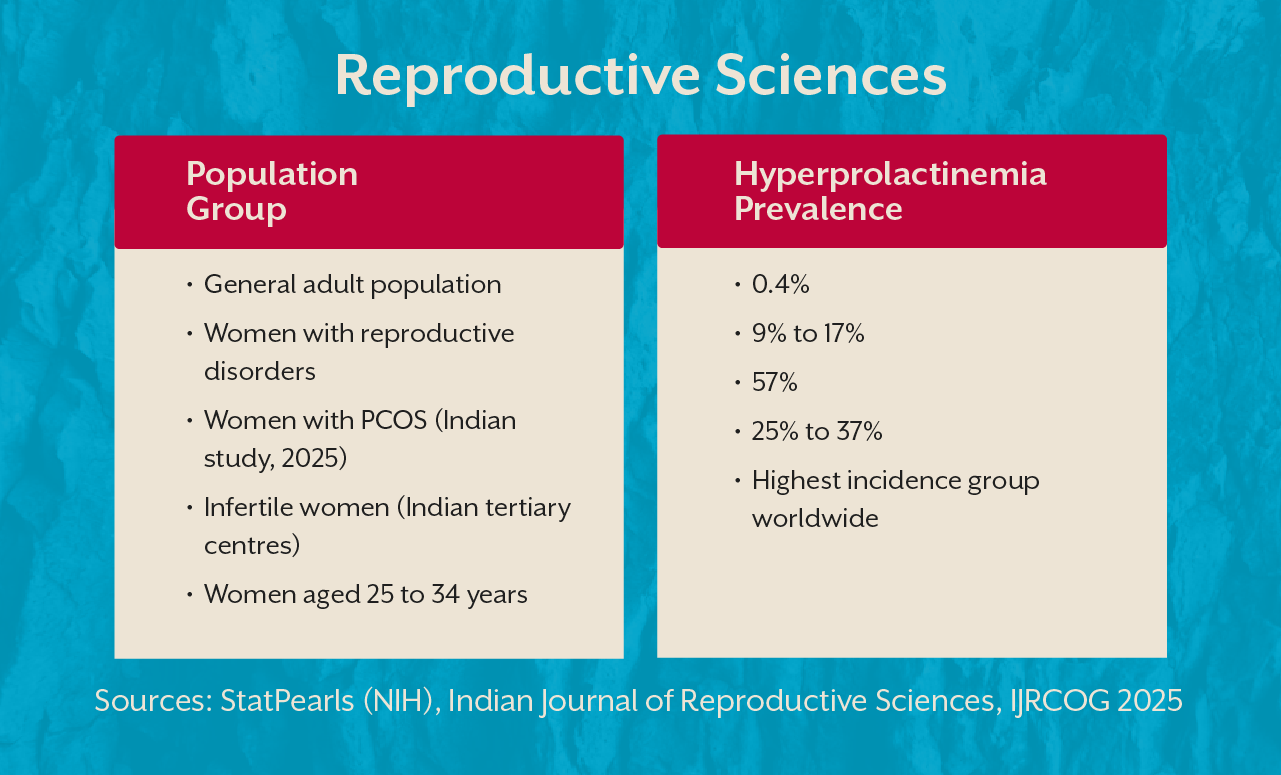
This is not a rare story. Research shows that between 25 and 37% of women presenting with unexplained infertility have elevated prolactin levels, yet a prolactin test is still not universally included in early hormonal workups.
Hyperprolactinemia, chronically elevated prolactin, is one of the most underdiagnosed hormonal disruptions in women of reproductive age. It derails periods, blocks ovulation, feeds mood instability, and creates a confusing symptom picture that points in every direction except the right one.
How Common Is This? The Numbers That Should Alarm Us
Before diving into symptoms, it is worth pausing on how widespread this condition actually is in India.
That last row is particularly striking. In a 2025 Indian study of 110 women with PCOS, over half had hyperprolactinemia. These are not numbers from a rare endocrine condition. They are the everyday hormonal reality of Indian women.
What Is Hyperprolactinemia and Why Does It Hit Women Hardest
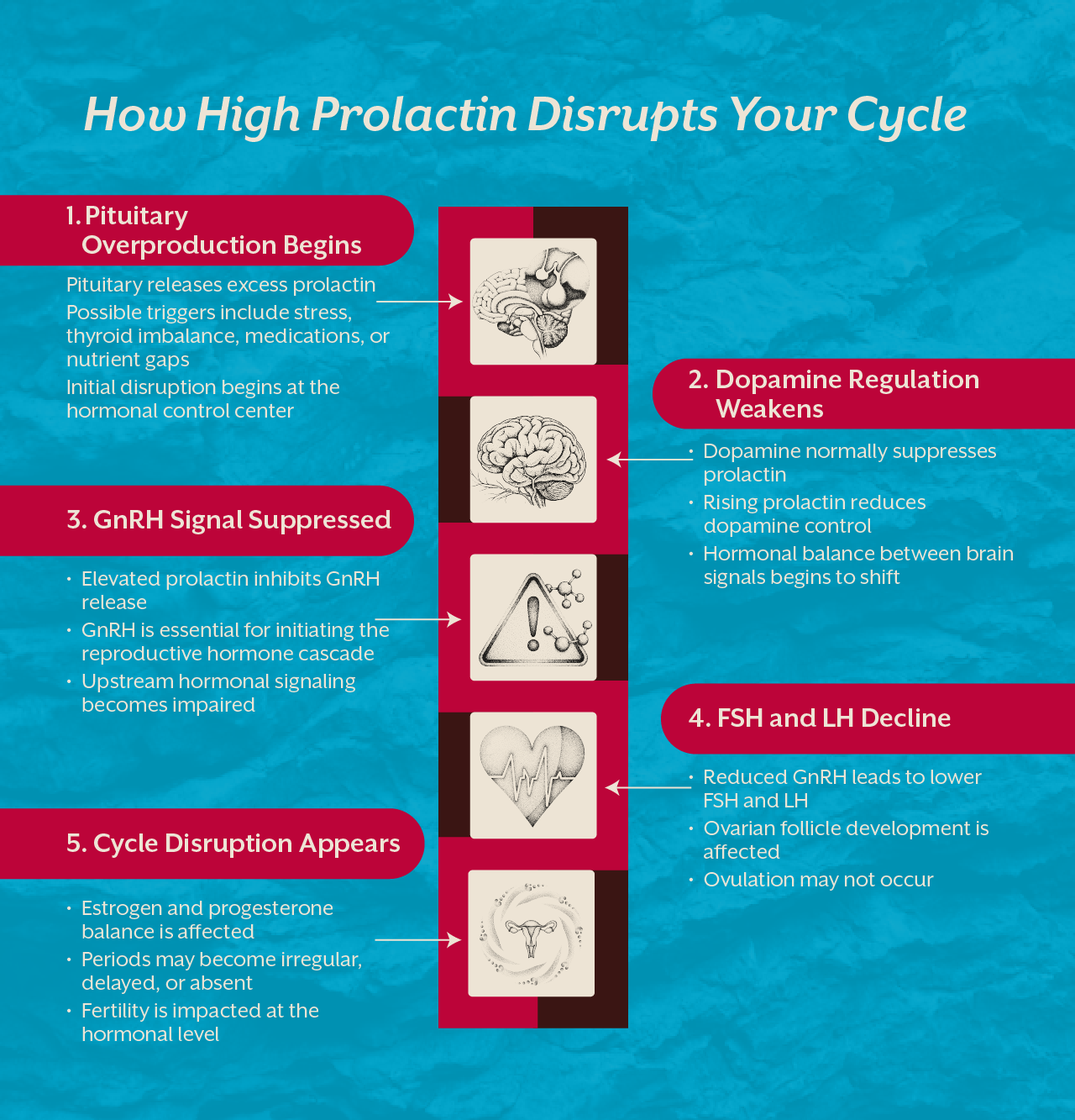
Prolactin is a hormone made by the pituitary gland. Its primary role is to trigger breast milk production after childbirth. Outside of pregnancy and nursing, prolactin should stay low. When it rises without a biological reason, the consequences are significant because prolactin directly suppresses FSH and LH, the two hormones that govern the menstrual cycle.
When prolactin climbs, FSH and LH fall. When FSH and LH fall, ovulation stops. And when ovulation stops, the period disappears or grows erratic. This is the central mechanism driving hyperprolactinemia symptoms in females, and why the period is always the first thing to go.
Women carry a far greater burden of this condition than men. The female hormonal system is simply more sensitive to prolactin fluctuations because the reproductive cycle depends on getting it right.
Hyperprolactinemia Causes: What Is Actually Driving Your Prolactin Up
The cause is not always the same and treatment depends entirely on finding the right driver.
Prolactinoma
The most common structural cause is a prolactinoma, a benign pituitary tumour that overproduces prolactin. These account for nearly half of all pathological cases and are more common in women than men. Women typically develop smaller microprolactinomas that are harder to detect on routine imaging, which is one reason diagnosis is so often delayed.
Hypothyroidism
When the thyroid is underactive, excess TRH directly stimulates prolactin secretion. A woman with poorly managed hypothyroidism may have elevated prolactin purely as a downstream consequence. Treating the thyroid often normalises prolactin entirely, without any direct prolactin intervention at all.
Medications
Antipsychotics, certain antidepressants, blood pressure medications, and antiemetics raise prolactin by blocking dopamine, the brain chemical that normally keeps prolactin suppressed. This dopamine connection is central to understanding the condition and why nutritional support can genuinely make a difference.
Chronic Stress and Sleep Disruption
Prolactin rises with physical stress, poor sleep, and sustained high cortisol. Women who are consistently overworked and under-rested often carry mild to moderate prolactin elevation that nobody connects to their symptoms. The overlap with burnout is real. Read our blog on Addison's Disease Symptoms in Women Mistaken for Burnout for a fuller picture of how stress-related hormonal conditions disguise themselves.
Hyperprolactinemia Symptoms in Females: What Your Body Is Saying
Prolactin and Irregular Periods
The relationship between prolactin and irregular periods is direct. Elevated prolactin suppresses GnRH, which reduces FSH and LH from the pituitary. Without these signals, the ovaries do not ovulate. Periods arrive late, become very light, or stop entirely. The cycle irregularity is the symptom. Elevated prolactin is the cause.
Galactorrhea: Milk Without Pregnancy
One of the more startling high prolactin symptoms in women is galactorrhea, the spontaneous production of breast milk in a woman who is not pregnant or breastfeeding. This occurs in roughly one third to half of women with hyperprolactinemia. Many women notice it and stay silent, assuming it is normal. It is not. It is a direct sign that prolactin is biologically elevated and active.
Prolactin Fertility Problems
Elevated prolactin blocks ovulation and therefore blocks conception. Women who have been trying to conceive for over a year with irregular cycles should have prolactin tested as a first-line investigation. In Indian infertility studies, elevated prolactin was found in nearly 37% of women with endocrine-related infertility. Prolactin fertility interference is one of the most treatable causes of anovulatory infertility once properly identified.
Mood Shifts, Low Libido, and Brain Fog
Elevated prolactin suppresses estrogen, and low estrogen drives depression, poor libido, brain fog, and emotional flatness. Women describe a version of themselves they do not recognise: disinterested, flat, and disconnected. These are biological symptoms, not character changes. Some are placed on antidepressants that raise prolactin further, quietly worsening the very hormonal environment they are trying to correct.
The Dopamine Connection: Why This Is a Brain Chemistry Problem Too
Prolactin secretion is controlled primarily by dopamine, which is released continuously from the hypothalamus. Dopamine truly suppresses prolactin. When dopamine falls, prolactin rises promptly. This is not just pharmacology, rather it is nutritional biochemistry.
Dopamine synthesis requires tyrosine, vitamin B6, iron, and zinc. When a woman is chronically stressed, nutritionally depleted, or sleeping poorly, dopamine production suffers and prolactin climbs. Lifestyle and nutrition are not optional extras here. They sit directly at the root of the mechanism.
Think of dopamine as the valve and the prolactin as the water. When the valve is strong enough, the water stays controlled. When it weakens, everything overflows.
Hyperprolactinemia Natural Treatment: The Nutritional Foundation
Medical treatment through dopamine agonists is the clinical standard for prolactinomas. But for women with idiopathic or mildly elevated prolactin, targeted nutritional support can produce meaningful change. Hyperprolactinemia natural treatment is not a replacement for medical investigation. It is the biological foundation that makes any treatment more effective.
Vitamin B6
Vitamin B6 is a critical cofactor in dopamine synthesis. Studies have shown that B6 supplementation can minimise elevated prolactin in women with idiopathic hyperprolactinemia. Without adequate B6, the enzymatic step that converts tyrosine into dopamine cannot complete efficiently, and prolactin suppression weakens over time.
Zinc
Zinc plays a direct role in regulating pituitary function as well as prolactin release. Zinc deficiency impairs dopamine receptor sensitivity and has been linked to elevated prolactin. Women experiencing hair thinning or acne alongside cycle irregularity should have zinc status assessed as part of their hormonal investigation.
Hyperprolactinemia Diet: What to Build Your Plate Around
A hyperprolactinemia diet is a rebuilding plan, not a restriction list. Prioritise tyrosine-rich foods: eggs, chicken, nuts, and seeds. Add magnesium-rich foods like pumpkin seeds for dopamine receptor support. Include vitamin C rich fruits and vegetables to reduce oxidative stress at the pituitary level. Stable blood sugar is non-negotiable since cortisol spikes directly drive prolactin upward. Avoid alcohol, excessive caffeine, and ultra-processed foods that disrupt hypothalamic signalling.
What Actually Confirms Hyperprolactinemia
Diagnosis begins with a fasting morning serum prolactin test, drawn at least 2 hours after waking and before any physical exertion. A single elevated reading is not sufficient for diagnosis. A second confirmatory test is needed before any treatment decision is made.
If prolactin remains elevated, a pituitary MRI is ordered to check for adenoma. Thyroid function and medication history are reviewed simultaneously. Finding the root cause, rather than simply suppressing the number, determines whether treatment will hold.
If you are experiencing irregular periods, unexplained infertility, or mood disruption alongside cycle changes, a root cause analysis can map the full hormonal picture rather than treating each symptom in isolation.
Key Takeaway
Hyperprolactinemia is not rare. It is one of the most common hormonal conditions in Indian women of reproductive age, hiding behind missed periods, unexplained infertility, and mood changes written off as stress for years.
A single prolactin blood test can begin to change an entire diagnostic story. Whether the driver is a pituitary adenoma, an underactive thyroid, B6 and zinc deficiency, or chronic dopamine depletion, this condition has clear mechanisms and clear pathways of support. It goes undertreated not because it is complex, but because it goes untested.
If your hormonal picture feels incomplete and the standard answers are not adding up, do not wait. Book a consult and let the right investigation finally begin.
Star Your Root Cause Analysis
Includes home blood sample collection, 1-hour expert consultation, and a next-step protocol.


.svg)
.svg)