1 in 4 Indians Experiences Acid Reflux Regularly. Most Are Managing It With Antacids but You Have the Key to Reverse It.
Book Your Root Cause Analysis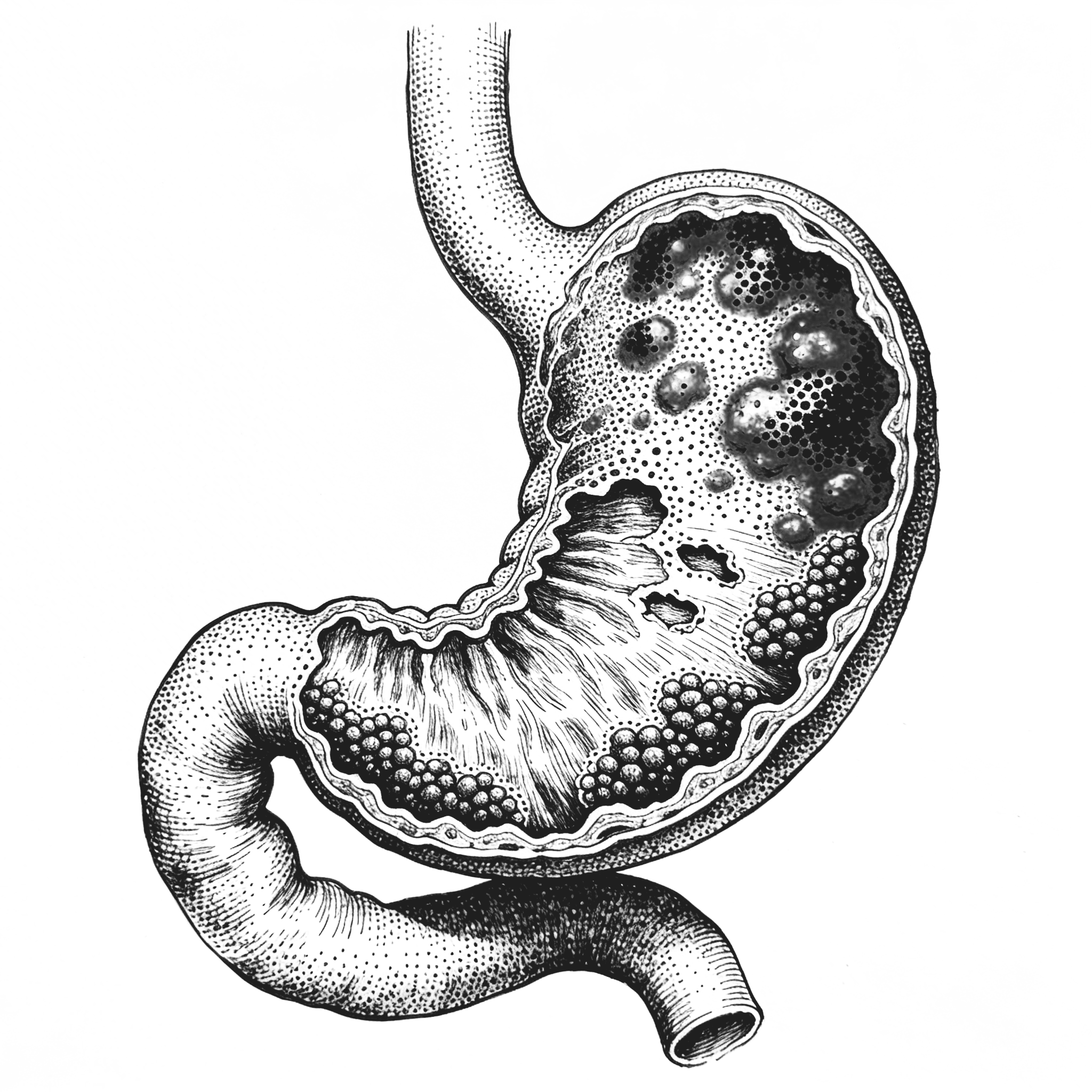
If You See Yourself Here, Don't Ignore It












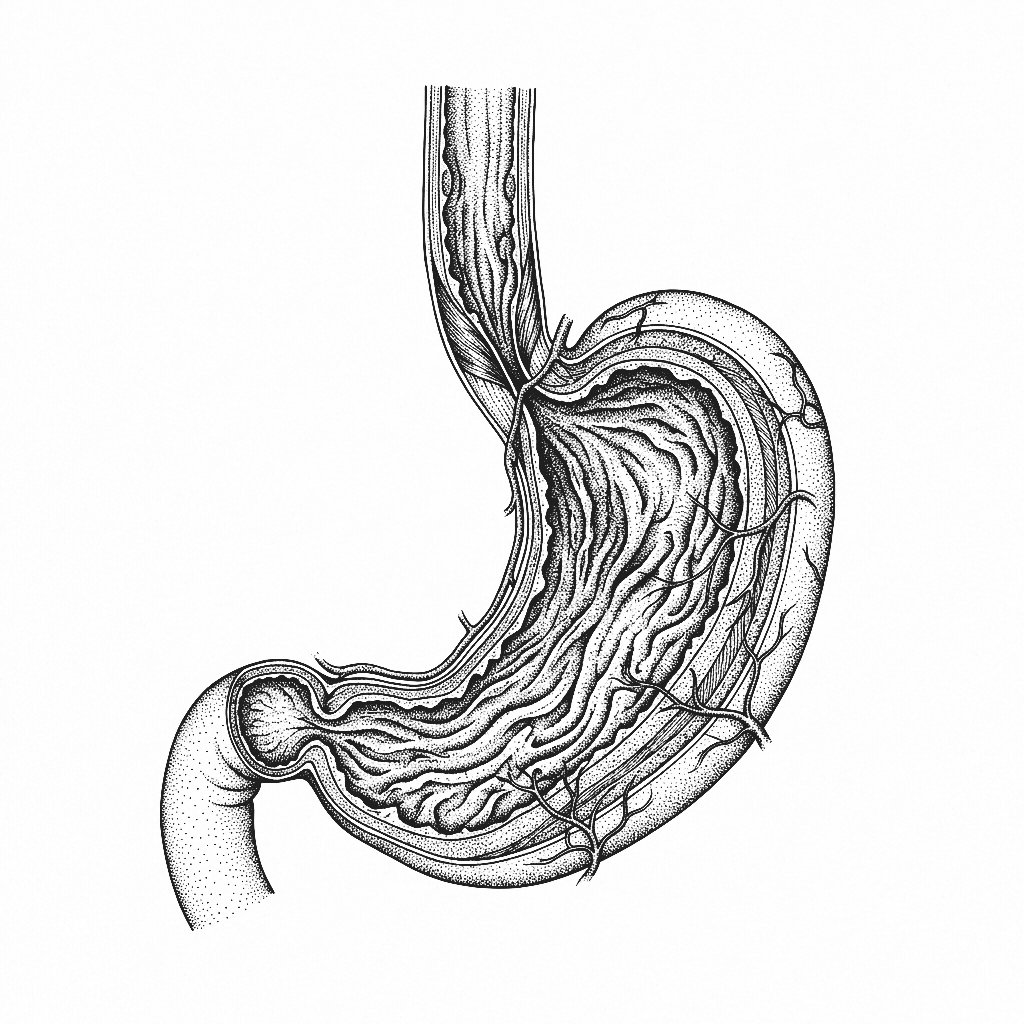
Acid Reflux Isn't What You Think It Is

Acid reflux occurs when stomach contents flow back up into the oesophagus, the tube connecting the mouth to the stomachstomach. When this happens frequently it becomes Gastroesophageal Reflux Disease or GERD. The conventional explanation is that the stomach produces too much acid. This is almost always incorrect. In most cases the problem is not the amount of acid but the failure of the lower oesophageal sphincter, the valve between the oesophagus and stomach to close properly. Stomach acid, which is supposed to stay in the stomach, travels upward and damages the oesophageal lining because it has no protective mucus layer. The burning is real. The cause is almost always mislabelled.
In the majority of cases acid reflux is driven by too little stomach acid, not too much. Low stomach acid, a condition called hypochlorhydria impairs digestion, causes food to ferment and produce gas in the stomach, and creates upward pressure that forces the lower oesophageal sphincter open. Add to this a disrupted gut microbiome, food sensitivities triggering inflammation in the oesophageal lining, a hiatal hernia in some cases, and chronic stress impairing digestive function and the picture becomes clear. Suppressing acid with PPIs removes the symptom while leaving every one of these drivers completely unaddressed.
India's dietary patterns create near-perfect conditions for GERD. Diets high in refined carbohydrates and low in diverse fibre disrupt the gut microbiome and impair digestion. Large meal portions eaten quickly, high consumption of spicy and fried foods, late night eating, widespread H. pylori infection which directly disrupts stomach acid regulation, chronic stress, and increasing rates of obesity all converge to make acid reflux one of the most prevalent digestive complaints in the country. Antacid and PPI use in India is among the highest in the world - and rising without any meaningful reduction in prevalence.
Long term PPI uses the standard treatment for GERD that suppresses stomach acid which is essential for mineral absorption, protein digestion, protection against gut infections, and microbiome balance. People on PPIs for years are frequently developing B12 deficiency, magnesium deficiency, iron deficiency, gut dysbiosis, and increased susceptibility to infection, all driven by the medication prescribed to manage their symptoms. The root cause remains active while the treatment creates an expanding list of secondary problems.
The Difference Between Managing Acid Reflux and Reversing It
CONVENTIONAL MEDICINE
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
FUNCTIONAL NUTRITION
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
Acid Reflux Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
CONSEQUENCES OF NOT ADDRESSING IT
74% of clients reported measurable reduction in reflux frequency, bloating, and post-meal discomfort within the first 60 days of their personalised protocol without increasing their medication.
What Real Acid Reflux Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of Acid Reflux and GERD

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
Long term PPI use significantly impairs the absorption of B12, magnesium, iron, and calcium, all of which require stomach acid to be properly absorbed. It also disrupts the gut microbiome and increases susceptibility to gut infections including C. difficile. PPIs manage the symptom while quietly creating a secondary set of deficiencies that worsen the overall picture over time.
For most people yes.. particularly when the root causes are identified and addressed. When stomach acid function is restored, H. pylori is cleared if present, gut permeability is repaired, and food triggers are identified and resolved, reflux very often resolves without ongoing medication.
Because trigger avoidance reduces irritation to an already damaged system but does not address why the system is failing. Low stomach acid, dysbiosis, gut permeability, and food immune reactivity are all still active regardless of what you remove from your diet. The underlying dysfunction needs to be addressed directly.
In the majority of cases yes. Low stomach acid causes fermentation and gas production in the stomach which creates upward pressure forcing the oesophageal valve open. The burning sensation is identical whether the cause is excess or insufficient acid which is why the distinction requires testing rather than assumption.
Because lying down removes the gravitational barrier that helps keep stomach contents in place during the day. Night-time reflux is typically a sign that the lower oesophageal sphincter tone is significantly impaired and that the underlying drivers like dysbiosis, food reactivity, and low acid are substantial enough that positional changes alone cannot compensate.






Talk to our team

Talk to our team
Download Now
