Esophagitis Is More Than Just Acid Damage. Most People Being Treated for It Have Never Had Its Real Drivers Investigated.
Book Your Root Cause Analysis
If You See Yourself Here, Don't Ignore It












Esophagitis Isn't What You Think It Is

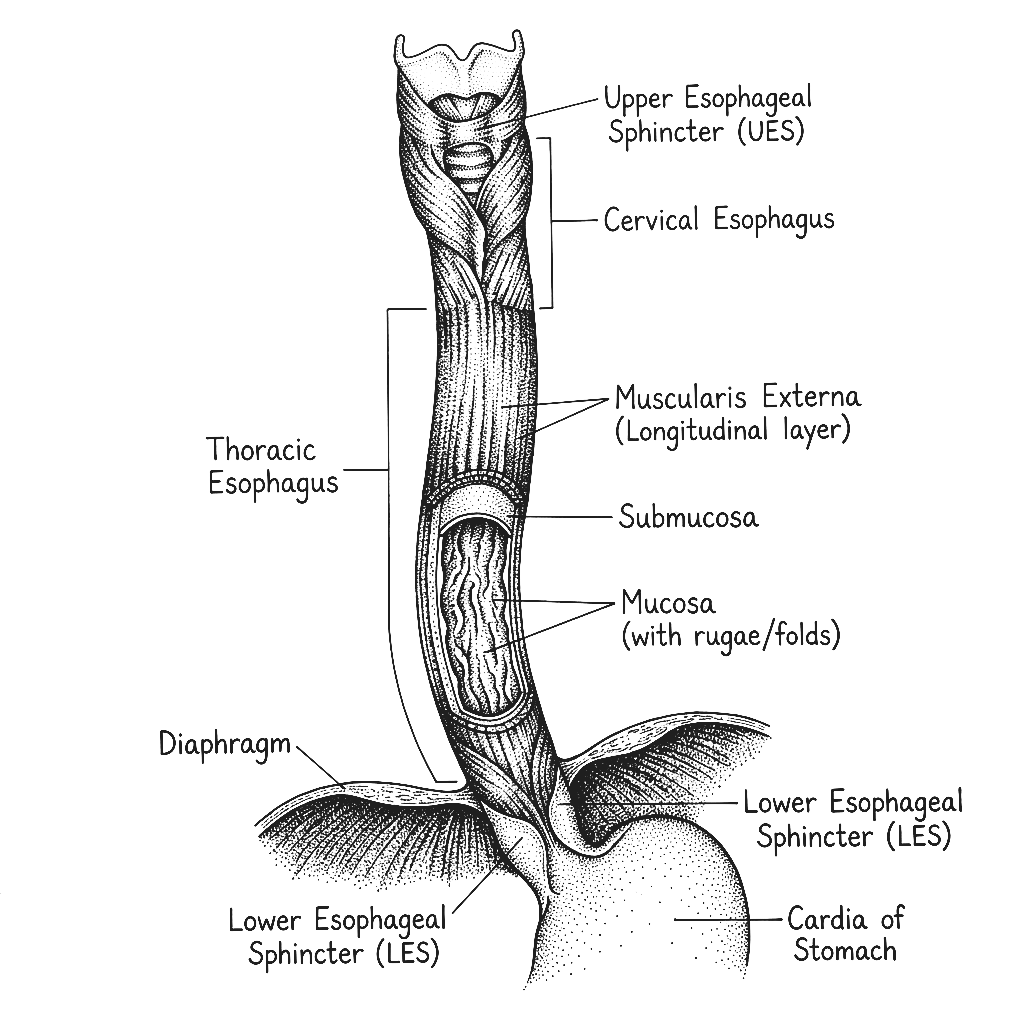
Esophagitis is inflammation of the oesophagus, the muscular tube that carries food and liquid from the mouth to the stomach. Unlike GERD which describes the mechanical reflux of stomach contents, esophagitis describes the actual tissue damage and inflammation that results from that reflux or from other triggers. The oesophageal lining has no protective mucus layer and is highly vulnerable to damage from acid, bile, immune-mediated inflammation, infection, and certain medications. When inflammation becomes chronic it causes the tissue changes, scarring, and structural damage that make swallowing progressively more painful and difficult. Esophagitis is not simply acid irritation. It is active tissue damage that requires the underlying drivers to be identified and addressed amd not just suppressed.
Esophagitis presents in several distinct forms each with different primary drivers. Reflux esophagitis is the most common and is caused by chronic acid or bile reflux damaging the oesophageal lining. Eosinophilic esophagitis is an immune-mediated condition in which eosinophils, a type of white blood cell accumulate in the oesophageal tissue in response to food allergens or environmental triggers, causing significant inflammation independent of acid. Infectious esophagitis can be caused by candida, herpes, or cytomegalovirus particularly in people with compromised immunity. Medication-induced esophagitis occurs when certain tablets or capsules lodge in the oesophagus and cause direct chemical damage. Identifying the type is essential because the drivers and the approach differ substantially between them.
Eosinophilic esophagitis also known as EoE is one of the most underdiagnosed conditions in gastroenterology in India. Its symptom picture overlaps almost entirely with GERD and reflux esophagitis, meaning it is frequently treated with PPIs that have no effect on the underlying immune mechanism driving it. EoE is driven by food and environmental allergens triggering an abnormal immune response in the oesophageal tissue and without specific biopsy and allergen investigation, it is never identified. A significant proportion of people who don't respond to standard acid suppression treatment have EoE as their actual diagnosis.
Rising rates of GERD driven by dietary and lifestyle factors, increasing prevalence of food sensitivities and immune dysregulation, high rates of H. pylori infection disrupting the gastric environment, widespread PPI use that alters the microbiome and impairs mucosal immunity, and low awareness of eosinophilic esophagitis as a distinct entity all contribute to a growing burden of esophagitis that is frequently mismanaged. The downstream consequences including Barrett's oesophagus, strictures, and progressive swallowing difficulty are significantly more common than they need to be given how addressable the root causes are.
Esophagitis is treated almost universally as an acid problem. For a significant proportion of patients it is an immune problem, a microbiome problem, a food sensitivity problem, or a combination of all three. Acid suppression addresses one mechanism while leaving the others completely unaddressed which is why so many people on long term PPIs continue to have symptoms, continue to sustain oesophageal damage, and continue to progress toward more serious structural changes. The question is not how to suppress acid more effectively. It is what is driving the inflammation in the first place.
The Difference Between Suppressing Esophagitis and Reversing It
CONVENTIONAL MEDICINE
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
FUNCTIONAL NUTRITION
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
Esophagitis Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
CONSEQUENCES OF NOT ADDRESSING IT
71% of clients with esophagitis reported measurable reduction in swallowing difficulty, chest discomfort, and reflux frequency within the first 50 days of their personalised protocol without increasing their medication.
What Real Esophagitis Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of Esophagitis

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
Because PPIs address acid as a single mechanism while leaving the other drivers of oesophageal inflammation involving immune activation, food sensitivities, dysbiosis, and mucosal damage completely unaddressed. If your esophagitis is eosinophilic or driven significantly by immune and gut factors, acid suppression alone will never be sufficient. The right investigation determines which mechanisms are actually driving your specific case.
Eosinophilic esophagitis is an immune-mediated condition in which specific white blood cells accumulate in the oesophageal lining in response to food or environmental allergens. It produces a symptom picture almost identical to reflux esophagitis but does not respond to acid suppression. Diagnosis requires oesophageal biopsy combined with food allergen and immune reactivity testing, neither of which is part of a standard GERD workup.
The oesophageal lining has meaningful capacity to repair when the inflammatory drivers are removed and the right nutritional support is provided. Early stage mucosal damage is highly reversible. More advanced changes including strictures and Barrett's oesophagus require more careful management but even in these cases addressing the root causes prevents further progression and supports whatever healing capacity remains.
Very commonly yes, particularly in eosinophilic esophagitis where food allergens are a primary driver. But even in reflux esophagitis, IgG-mediated food reactions drive gut permeability and inflammation that worsen oesophageal mucosal vulnerability. Identifying and addressing food immune triggers is a core component of any meaningful approach to esophagitis.
Yes and this is precisely why addressing the root causes now matters. Barrett's oesophagus is a pre-cancerous change in the oesophageal lining driven by chronic uncontrolled inflammation. Its progression is not inevitable, it depends on whether the inflammatory drivers are controlled. Addressing those drivers through a targeted root cause approach is the most meaningful thing that can be done to reduce the risk of further progression.






Talk to our team

Talk to our team
Download Now
