Food Sensitivities Affect Millions of People in India. Most Have No Idea Which Foods Are Driving Their Symptoms.
Book Your Root Cause Analysis
If You See Yourself Here, Don't Ignore It












Food Sensitivities Aren't What You Think They Are

Food sensitivities are delayed immune reactions to specific foods, distinct from food allergies which are immediate IgE-mediated responses, and distinct from food intolerances which are enzyme-based digestive failures. Food sensitivities involve IgG and IgA mediated immune reactions that can occur hours or even days after consumption, making the connection between food and symptom extremely difficult to identify without specific testing. The reactions are real, measurable, and physiological. They are not pickiness, psychological, or a matter of willpower. They are the immune system mounting a response to food particles it has been incorrectly trained to recognise as threats almost always as a consequence of underlying intestinal permeability.
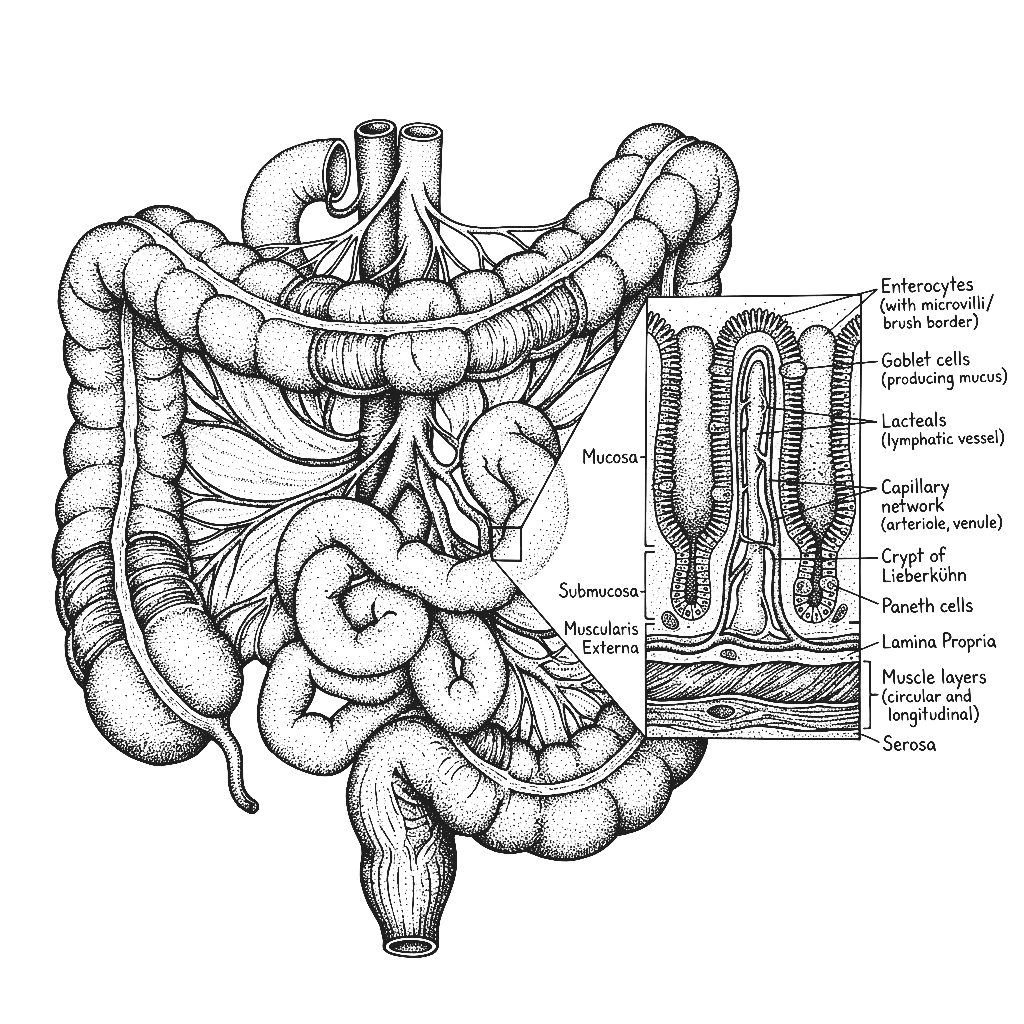
A healthy gut barrier prevents undigested food particles from entering the bloodstream. When intestinal permeability develops through dysbiosis, chronic stress, NSAID use, dietary patterns, or gut infections, food particles cross into the bloodstream before they are fully broken down. The immune system encounters these particles and mounts a response, creating antibodies against them. Every subsequent exposure to that food triggers an immune reaction. This is why food sensitivities are almost always a downstream consequence of leaky gut rather than a standalone condition and why eliminating trigger foods without repairing the gut barrier only provides partial and temporary relief.
Standard allergy testing checks for IgE antibodies, the immediate hypersensitivity response. Food sensitivities involve IgG and IgA antibodies which are not assessed in routine allergy panels. A person can test completely negative on a standard allergy panel and still have significant IgG-mediated reactions to multiple foods driving chronic symptoms. This is why so many people with clear food-related symptoms are told their tests are normal and sent away without answers, the right antibodies were never measured.
High rates of gut dysbiosis, widespread intestinal permeability driven by dietary patterns and chronic stress, a medical system that does not routinely test for IgG food reactions, and diets that expose the gut to the same foods repeatedly without rotation, all of these create conditions in which food sensitivities develop commonly and go unidentified for years. The most frequently reactive foods in the Indian population include wheat, dairy, eggs, certain legumes, and specific spices the staples consumed daily, making the connection to symptoms even harder to identify without testing.
Food sensitivities are not the root problem. They are the signal that the gut barrier has been compromised and the immune system has lost appropriate tolerance. Identifying and removing trigger foods provides symptom relief but the sensitivity list will continue to expand unless the underlying intestinal permeability and immune dysregulation are addressed directly. Fix the gut and the immune system very often regains tolerance to foods it was previously reacting to.
The Difference Between Avoiding Foods and Fixing the System
CONVENTIONAL MEDICINE
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
FUNCTIONAL NUTRITION
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
Food Sensitivities Aren't One Problem. They're Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as Food Sensitivities Doesn't End There

75% of clients with multiple food sensitivities reported measurable reduction in reactions, improved digestive comfort, and successful reintroduction of previously reactive foods within the first 45 days of their personalised protocol.

What Real Food Sensitivity Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of Food Sensitivities

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
No. Standard allergy tests measure IgE antibodies which detect immediate hypersensitivity reactions. Food sensitivities involve IgG and IgA antibodies which are delayed reactions occurring hours or days after eating and are not measured in routine allergy panels. A negative allergy test does not rule out food sensitivities, it simply means a different type of immune reaction needs to be assessed.
For most people the sensitivities can be significantly reduced or resolved when the underlying intestinal permeability and immune dysregulation are addressed. As the gut barrier is repaired and the immune system regains appropriate tolerance, previously reactive foods can often be successfully reintroduced. Permanent elimination of multiple foods is a management strategy, not a solution.
Because the underlying gut permeability driving the sensitivities has never been addressed. Every new food that crosses a compromised gut barrier becomes a potential new target for immune sensitisation. The expanding list is not random, it is the immune system continuing to react to an ongoing barrier failure. Repair the barrier and the expansion stops.
Very commonly yes. IgG mediated food reactions drive systemic inflammation that manifests on the skin particularly as acne, eczema, rosacea, and urticaria. Skin conditions that have not responded to topical treatment are frequently driven by dietary immune triggers that have never been identified through the right testing.
An elimination diet removes suspected foods based on common triggers or symptom patterns without identifying the specific immune reactions present. It can provide partial relief but misses reactions to unexpected foods and provides no information about gut permeability, immune dysregulation, or how to systematically reintroduce foods. Specific IgG testing combined with gut assessment gives a complete picture that an elimination diet cannot replicate.






Talk to our team

Talk to our team
Download Now
