1 in 5 People Has IBS. Most Are Managing It but You Have the Key to Reverse It.
Book Your Root Cause Analysis.png)
If You See Yourself Here, Don't Ignore It












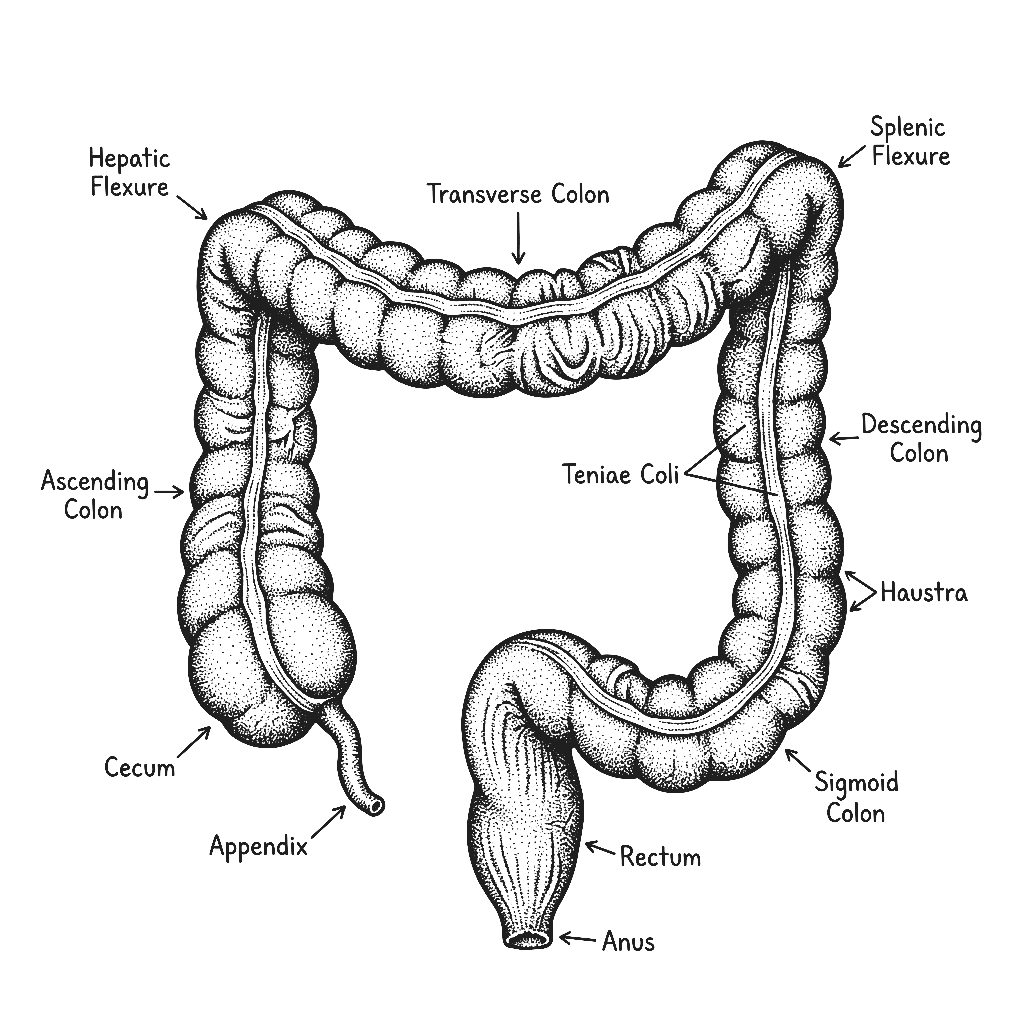
IBS Isn't What You Think It Is

Irritable Bowel Syndrome is a functional gut condition characterised by chronic abdominal discomfort, altered bowel habits, and digestive symptoms that significantly affect daily life. It is not a disease of visible structural damage, colonoscopies and scans come back normal which is precisely why it is so often dismissed. But normal on imaging does not mean nothing is wrong. IBS reflects a breakdown in the communication between the gut, the nervous system, the microbiome, and the immune system. The gut is dysfunctional at a level that standard investigations simply aren't designed to detect.
IBS presents three main patterns.
- IBS-D is diarrhoea predominant, characterised by frequent loose stools and urgency.
- IBS-C is constipation predominant, with infrequent, difficult, or incomplete evacuation.
- IBS-M is a mixed type, alternating between both.
Understanding which pattern is present matters because the root causes driving each can differ and the protocol needs to be built around the specific pattern and its underlying drivers, not a generic gut supplement stack.
India has one of the highest rates of IBS in the world and it is increasing. Diets high in refined carbohydrates and low in diverse fibre, widespread antibiotic use disrupting the microbiome, chronic psychological stress directly impairing gut motility and permeability, high rates of prior gut infections including parasitic and bacterial, widespread Vitamin D deficiency, and food adulteration all converge to create near-perfect conditions for IBS to develop and persist. It is not a condition of weak constitution. It is a condition of a gut system under sustained pressure without the right support.
IBS is almost never just a gut problem. The gut-brain axis, the bidirectional communication network between the digestive system and the central nervous system is almost always involved. So is the microbiome, gut permeability, low-grade immune activation, and in many cases an underlying condition like SIBO or food sensitivity that has never been identified. Treating IBS with fibre advice and antispasmodics without investigating these drivers is why so many people manage symptoms for years without ever actually improving.
The Difference Between Managing IBS and Reversing It
CONVENTIONAL MEDICINE
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
FUNCTIONAL NUTRITION
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
IBS Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as IBS Doesn't End There

72% of clients reported measurable reduction in bloating, cramping, and bowel irregularity within the first 60 days of their personalised protocol.
What Real IBS Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
The Solution Always Includes

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
A normal colonoscopy rules out structural disease like cancer or IBD. It does not assess microbiome composition, gut permeability, food immune reactions, SIBO, or the gut-brain axis, all of which are common drivers of IBS. Normal on a colonoscopy and normal gut function are not the same thing.
For most people, yes particularly when the specific root causes are identified and addressed. When dysbiosis is corrected, gut permeability is restored, and food triggers are identified and resolved at the immune level rather than just avoided, symptoms very often resolve rather than simply being managed.
Directly, but the relationship runs both ways. Chronic stress impairs gut motility, increases permeability, and alters the microbiome. But gut dysfunction also drives anxiety through the gut-brain axis, so stress and IBS reinforce each other. Addressing the gut biology very often improves the psychological symptoms alongside the physical ones.
Because low FODMAP reduces fermentable substrates and can relieve symptoms temporarily but it does not address why the gut is reacting to those foods in the first place. It is a symptom management tool, not a root cause solution. Without addressing dysbiosis, permeability, and immune reactivity, the underlying dysfunction remains active.
Very possibly. SIBO is present in a significant proportion of IBS cases and produces an identical symptom picture. Food sensitivities particularly non-IgE mediated reactions that don't show on standard allergy tests are also a common driver. Both require specific functional testing to identify and neither is part of a standard gastroenterology workup.






Talk to our team

Talk to our team
Download Now
