SIBO Is One of the Most Underdiagnosed Gut Conditions in India. Most People Who Have It Have Never Heard of It.
Book Your Root Cause Analysis.png)
If You See Yourself Here, Don't Ignore It












SIBO Isn't What You Think It Is

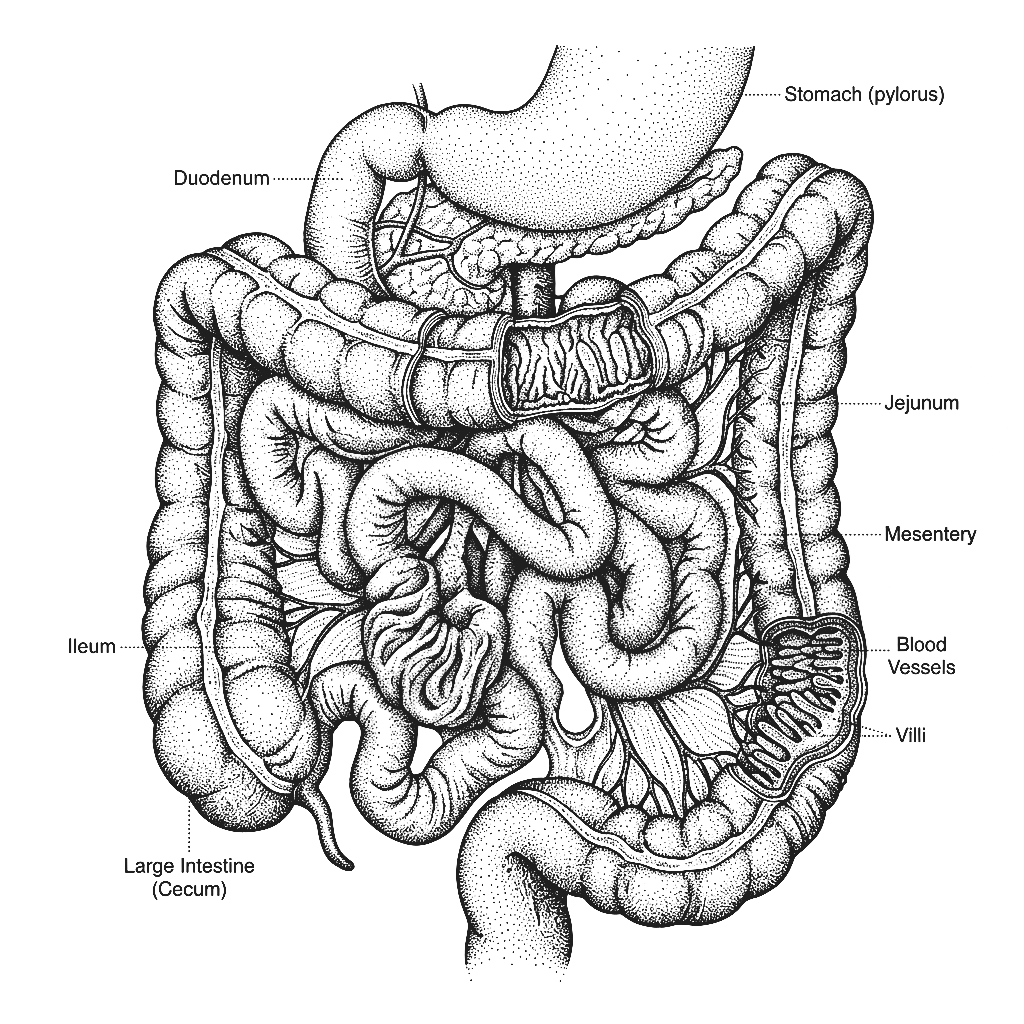
Small Intestinal Bacterial Overgrowth is a condition in which bacteria that should be confined largely to the large intestine migrate into and colonise the small intestine in abnormally high numbers. The small intestine is designed for nutrient absorption, not bacterial fermentation. When bacteria take up residence there they ferment carbohydrates before they can be properly digested, producing hydrogen or methane gas that causes the characteristic bloating, distension, and discomfort associated with the condition. They also damage the intestinal lining, impair nutrient absorption, and produce toxic byproducts that affect the entire body well beyond the gut. SIBO is not a minor inconvenience. It is a significant disruption to the body's primary nutrient absorption organ.
SIBO presents in three main forms depending on which gases the overgrown bacteria produce. Hydrogen-dominant SIBO typically causes diarrhoea, bloating, and cramping. Methane-dominant SIBO technically now referred to as Intestinal Methanogen Overgrowth or IMO tends to cause constipation, bloating, and slower motility. Hydrogen sulphide SIBO is less commonly tested for but associated with diarrhoea, a sulphurous odour, and significant gut inflammation. Each type has different drivers and requires a different therapeutic approach which is why a single antibiotic course without identifying the type and underlying cause has such a high recurrence rate.
SIBO is almost never tested for in standard gastroenterology practice in India. The breath test required for diagnosis is not part of routine investigation and awareness among clinicians is limited. The symptom picture involving bloating, altered bowel habits, and fatigue is almost universally attributed to IBS, stress, or dietary intolerance without any investigation into whether bacterial overgrowth is the underlying driver. Studies suggest SIBO is present in a significant proportion of people diagnosed with IBS, meaning a large number of people in India are being managed for the wrong condition entirely.
SIBO is almost never the starting problem. It is the result of something that has compromised the small intestine's natural defence against bacterial overgrowth typically impaired gut motility, low stomach acid, a damaged ileocecal valve, or prior gut infection or antibiotic use. Treating SIBO with antibiotics without identifying and addressing these underlying drivers is why recurrence rates are so high. The bacteria return because the conditions that allowed them to colonise in the first place have never been corrected.
The Difference Between Treating SIBO and Reversing It
CONVENTIONAL MEDICINE
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
FUNCTIONAL NUTRITION
- Basic blood panel: LH, FSH, total testosterone
- Ultrasound to check for follicles
- Oral contraceptive pill to stimulate cycles
- Metformin for insulin resistance
- Advice to lose weight and manage stress
SIBO Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as SIBO Doesn't End There
76% of clients with SIBO reported measurable reduction in bloating, bowel irregularity, and fatigue within the first 60 days of their personalised protocol without requiring repeat antibiotic courses.
What Real SIBO Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of SIBO

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
Because antibiotic treatment clears the overgrowth temporarily but does not address why the bacteria were able to colonise the small intestine in the first place. Low stomach acid, impaired motility, a damaged ileocecal valve, or gut dysbiosis all remain active after treatment. Until these are identified and corrected, recurrence is almost inevitable.
Very possibly. SIBO produces a symptom picture almost identical to IBS such as bloating, altered bowel habits, cramping, and fatigue. Studies consistently show SIBO is present in a significant proportion of people diagnosed with IBS. If your IBS has never responded meaningfully to treatment, SIBO is one of the first things that should be investigated.
Yes and this is one of the most underappreciated consequences. Bacterial overgrowth in the small intestine directly competes for nutrients before they can be absorbed particularly B12, iron, and fat soluble vitamins. People with long standing SIBO frequently present with deficiencies that don't respond to supplementation because the absorption problem has never been addressed.
In some cases yes. Introducing additional bacteria into an already overgrown small intestine can worsen symptoms which is why many people with SIBO find probiotics make them feel significantly worse. Probiotic use in SIBO needs to be carefully timed and targeted to the specific type of overgrowth and stage of treatment.
Directly. The gut-skin axis is well established and SIBO is specifically associated with rosacea, acne, and other inflammatory skin conditions. The bacterial overgrowth drives systemic inflammation and intestinal permeability that manifests on the skin. When SIBO is addressed, skin conditions that have been unresponsive to topical treatment very often improve significantly.






Talk to our team

Talk to our team
Download Now
