1 in 10 Indian Men Has Erectile Dysfunction. Most Are Just Handed a Pill and Sent Home.
Book Your Root Cause Analysis
If You See Yourself Here, Don't Ignore It












Erectile Dysfunction Isn't What You Think It Is

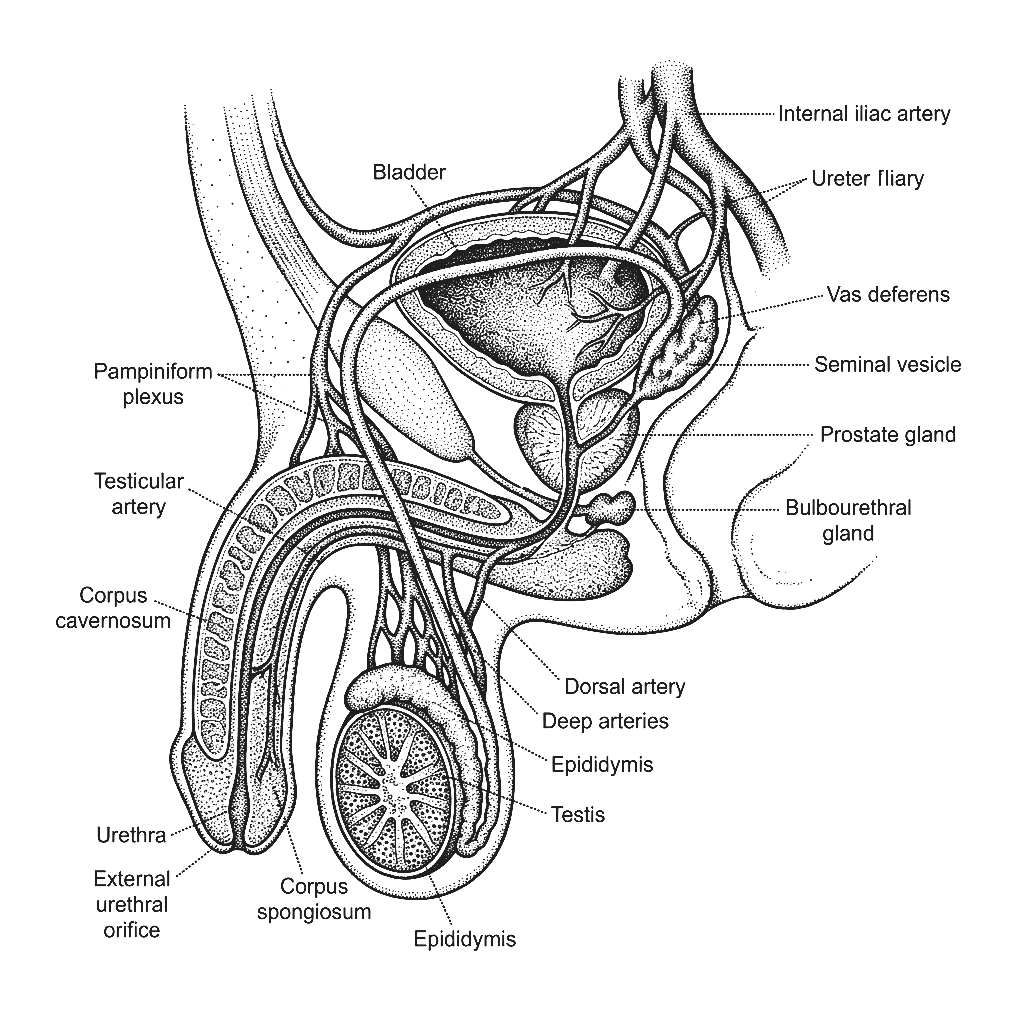
Erectile Dysfunction is the persistent inability to achieve or maintain an erection sufficient for satisfactory sexual activity. It is not a standalone condition, it is a symptom of underlying physiological dysfunction. An erection requires a precise coordination of hormonal signals, healthy blood flow, functioning nerve pathways, and metabolic balance. When any of these systems is compromised through insulin resistance, hormonal imbalance, cardiovascular dysfunction, or chronic inflammation the result shows up as ED. The erection is the signal. The root cause is elsewhere.
ED is significantly more prevalent in India than most men realise and it is getting younger. Urban Indian men face a convergence of metabolic risk factors: diets high in refined carbohydrates driving insulin resistance, sedentary desk-based work reducing cardiovascular fitness, chronic occupational stress elevating cortisol and suppressing testosterone, widespread Vitamin D deficiency, sleep deprivation, and increasing rates of obesity and type 2 diabetes all of which are direct physiological drivers of erectile dysfunction. ED in a man in his 30s or 40s is not bad luck, it is a metabolic signal.
ED is one of the earliest warning signs of cardiovascular and metabolic dysfunction often appearing 3 to 5 years before a cardiac event or diabetes diagnosis. The same endothelial damage that restricts blood flow to the heart restricts blood flow to the penis first. When a man presents with ED, the right question is not which pill will help, it is what is happening systemically that is impairing vascular and hormonal function. Address that, and erectile function often restores itself naturally.
The Difference Between Managing ED and Reversing It
CONVENTIONAL MEDICINE
- Prescription of PDE5 inhibitors
- Basic testosterone check
- Advice to exercise more and reduce stress
- No investigation into why testosterone is low or why blood flow is impaired
- No follow-up on metabolic or cardiovascular drivers
FUNCTIONAL NUTRITION
- Root Cause Analysis with 60+ Functional Markers
- Fasting insulin, HOMA-IR, full lipid panel, cardiovascular markers
- Free and total testosterone, SHBG, LH, FSH, oestradiol
- Inflammatory markers, gut health, complete nutrient status
- A dedicated functional nutritionist guides every step
ED Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as ED Doesn't End There
76% of clients reported measurable improvement in energy, drive, and erectile function within the first 60 days of their personalised protocol without medication changes.
What Real ED Reversal Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of ED

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
No. PDE5 inhibitors improve blood flow mechanically in the moment but they do not address why blood flow or hormonal function is impaired in the first place. Insulin resistance, low testosterone, endothelial inflammation, and nutrient deficiencies all remain active. The medication is a workaround, not a solution.
For most men, yes particularly when ED is driven by metabolic and hormonal root causes rather than structural damage. When insulin resistance is corrected, testosterone is restored, and cardiovascular function improves, erectile function very often restores itself naturally. Medication becomes unnecessary rather than mandatory.
Standard panels check total testosterone, not free testosterone, which is what the body actually uses. A total testosterone of 450 ng/dL looks normal but if SHBG is elevated, free testosterone may be critically low. Oestradiol, LH, FSH, and SHBG all need to be assessed together to understand the full hormonal picture.
Yes and this is important. ED in men under 45 is consistently associated with underlying cardiovascular and metabolic dysfunction. Research shows ED often precedes a cardiac event by 3 to 5 years. It is one of the body's earliest warning signals that something systemic needs attention. Addressing it early is not vanity, it is preventive health.
Directly. Weight gain, fatigue, and ED are very commonly downstream of the same root cause as insulin resistance drives low testosterone and elevated oestradiol. They feel like separate problems but they share the same origin. When that origin is addressed, all three typically improve together.






Talk to our team

Talk to our team
Download Now
