1 in 6 Couples in India Faces Fertility Challenges. Most Are Jumping Straight to IVF Without Ever Investigating Why.
Book Your Root Cause Analysis
If You See Yourself Here, Don't Ignore It












Fertility Challenges Aren't What You Think They Are

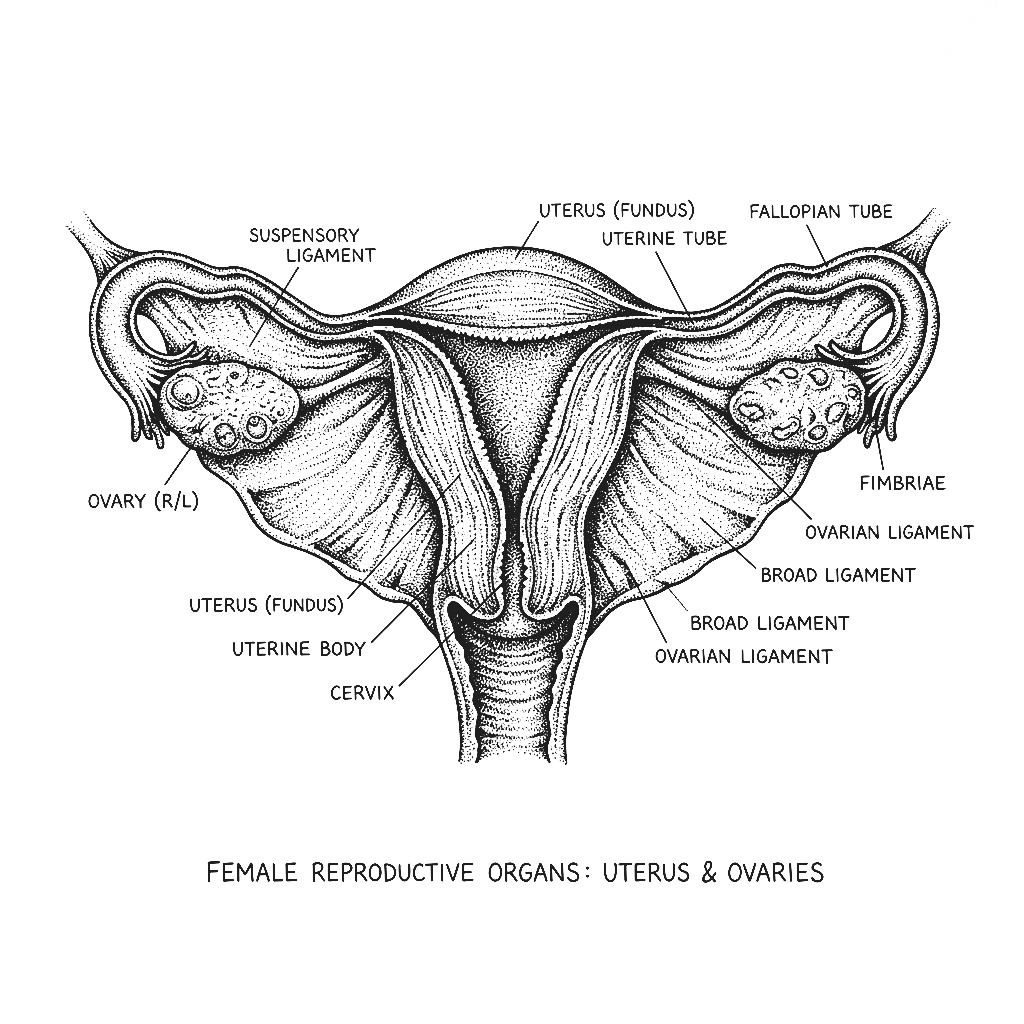
Fertility challenges refer to difficulty conceiving after twelve months of regular unprotected intercourse or six months for women over 35. They affect both partners equally approximately one third of cases involve female factors, one third involve male factors, and one third involve both or remain unexplained. The word unexplained is critical. In most cases unexplained infertility does not mean nothing is wrong. It means the standard investigations including semen analysis, ovarian reserve testing, and tubal patency assessment have not identified a structural cause. The functional drivers such as insulin resistance, subclinical thyroid dysfunction, nutrient deficiencies, gut health, oxidative stress, and hormonal imbalance are almost never investigated. They are almost always present.
Ovulation, implantation, and the maintenance of early pregnancy all require a precise hormonal environment. Insulin resistance drives androgen excess suppressing ovulation. Thyroid dysfunction impairs the hormonal signalling required for follicle development and implantation. Progesterone deficiency makes the uterine lining inhospitable to implantation. Elevated prolactin suppresses ovulation. Inflammation damages egg quality and disrupts the implantation environment. Every one of these is a functional driver of female infertility and every one of them is identifiable through specific testing yet standard fertility investigations address none of them comprehensively.
Male factor infertility accounts for approximately half of all fertility challenges yet receives a fraction of the investigative attention. A standard semen analysis assesses count, motility, and morphology but tells nothing about the oxidative stress that damages sperm DNA, one of the most significant drivers of both failed conception and recurrent miscarriage. Testosterone, LH, FSH, and oestradiol in men are rarely assessed. Nutrient deficiencies critical for sperm production such as zinc, selenium, CoQ10, vitamin D are almost never tested. The functional drivers of poor sperm quality are highly addressable yet consistently uninvestigated.
India has one of the highest rates of fertility challenges in the world and the age of first conception is rising. High rates of PCOS driven by insulin resistance, widespread thyroid dysfunction, significant rates of vitamin D deficiency impairing reproductive hormone function, chronic psychological stress disrupting the HPG axis, dietary patterns driving oxidative stress and poor egg and sperm quality, environmental toxic burden affecting hormonal regulation, and a fertility industry that moves quickly to assisted reproduction without investigating the functional terrain all contribute to a growing burden of fertility challenges that are more addressable than they are being addressed.
Fertility is not a standalone function. It is the output of metabolic health, hormonal balance, gut integrity, nutrient status, and immune regulation all working together. When any of these systems is compromised the reproductive system which is not essential for survival is one of the first to be downregulated. The body does not prioritise reproduction in an environment of metabolic stress, inflammation, and nutrient depletion. Addressing the environment and reproductive function very often restores itself naturally, without assisted reproduction.
The Difference Between Treating Infertility and Addressing Its Drivers
CONVENTIONAL MEDICINE
- Semen analysis, ovarian reserve testing, and tubal patency assessment
- Ovulation induction with Clomid or letrozole
- IUI as first line assisted reproduction
- IVF when other interventions fail
- Hormonal stimulation protocols without investigation into why hormones are dysregulated
- No assessment of insulin resistance, thyroid antibodies, nutrient status, or oxidative stress
FUNCTIONAL NUTRITION
- Root Cause Analysis with 60+ functional markers
- Full hormonal panel including LH, FSH, oestradiol, progesterone, prolactin, and testosterone
- Fasting insulin, HOMA-IR, and full thyroid panel including antibodies
- Oxidative stress and sperm DNA fragmentation markers
- Vitamin D, zinc, selenium, CoQ10, folate, and iron status
- Cortisol rhythm and adrenal function markers
- A dedicated functional nutritionist guides every step
Challenges Aren't One Problem. They're Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as Fertility Challenges Doesn't End There
71% of clients presenting with fertility challenges identified at least three addressable root causes in their Root Cause Analysis and reported measurable improvement in hormonal markers and cycle regularity within the first 60 days of their personalised protocol.
What Real Fertility Recovery Looks Like









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of Fertility Challenges

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
No. Unexplained infertility means the standard structural investigations have not found a cause, not that no cause exists. Functional drivers including insulin resistance, subclinical thyroid dysfunction, progesterone deficiency, nutrient deficiencies, oxidative stress, and gut permeability are almost never assessed in a standard fertility workup and are almost always present. Unexplained is a starting point for the right investigation, not a conclusion.
Ideally before because the factors that determine natural conception also determine IVF success. Egg quality, uterine receptivity, sperm DNA integrity, and hormonal environment all directly influence IVF outcomes and all are addressable through functional nutrition. Many couples who address root causes conceive naturally before reaching IVF. Those who do proceed to IVF do so with a significantly improved biological foundation.
Yes. Sperm production is a continuous process and new sperm are produced every 74 days. This means that improvements in the nutritional, hormonal, and oxidative stress environment translate directly into improved sperm quality within approximately three months. Zinc, selenium, CoQ10, vitamin D, and antioxidant status all directly influence sperm count, motility, morphology, and DNA integrity and are almost never assessed in standard male fertility investigation.
PCOS is one of the most common causes of ovulatory infertility but it is also one of the most responsive to root cause intervention. When insulin resistance is corrected, androgens normalise, and ovulation resumes often naturally and without ovulation induction medication. Many women with PCOS who address the underlying metabolic drivers conceive naturally once ovulatory function is restored.
Yes and this is critically underinvestigated. Recurrent miscarriage is associated with chromosomal abnormalities driven by poor egg quality from oxidative stress and mitochondrial dysfunction, progesterone deficiency impairing implantation maintenance, thyroid dysfunction, insulin resistance, immune dysregulation, and nutrient deficiencies including folate and vitamin D. Each of these is identifiable and addressable yet standard recurrent miscarriage investigations focus primarily on structural and chromosomal factors.






Talk to our team

Talk to our team
Download Now
