Millions of Indian Women Suffer Every Month Before Their Period. Most Are Told It's Just Part of Being a Woman.
Book Your Root Cause Analysis
If You See Yourself Here, Don't Ignore It











PMS Isn't What You Think It Is

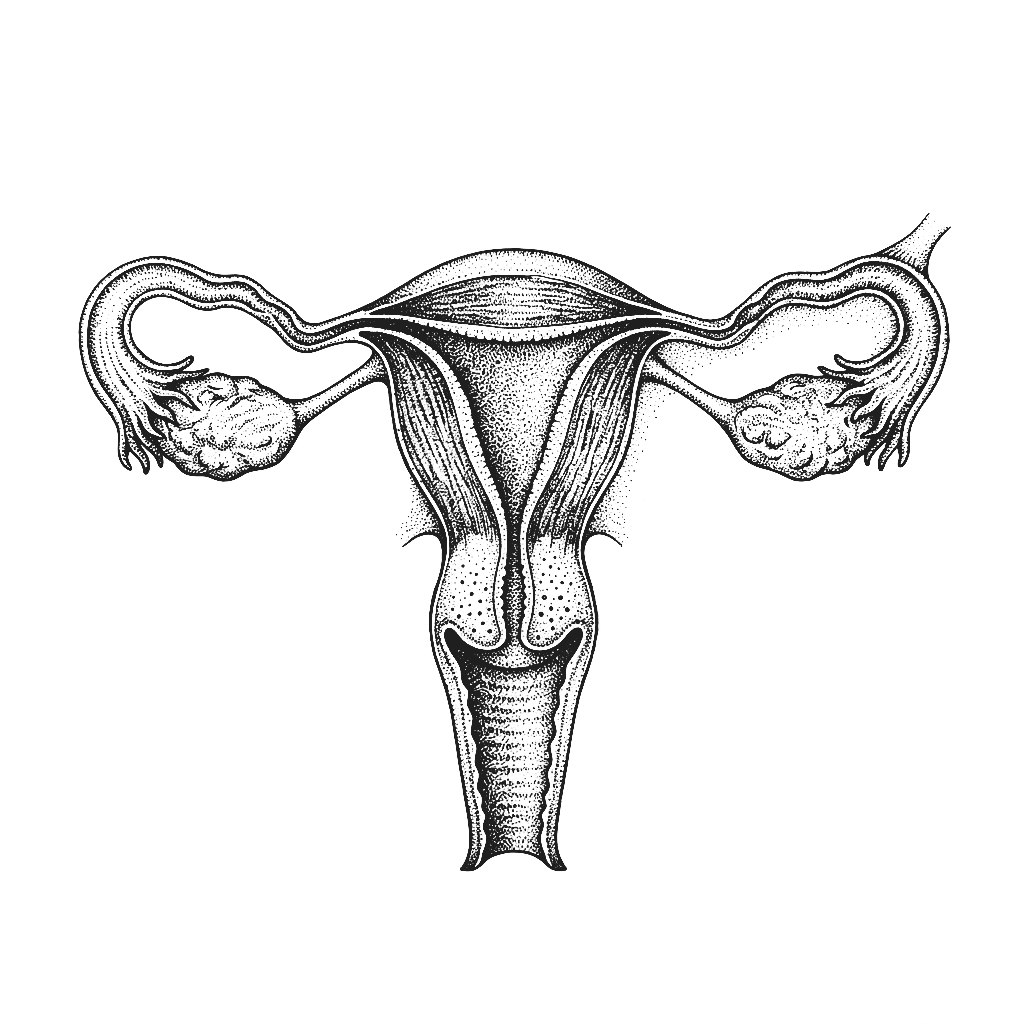
Premenstrual Syndrome is a pattern of physical, emotional, and behavioural symptoms that occur in the luteal phase of the menstrual cycle, the one to two weeks between ovulation and the start of menstruation and resolve within a few days of the period beginning. PMS is not simply the normal discomfort of having a period. It is a sign that the hormonal transition between the mid-cycle and menstruation is not happening smoothly, further driven by specific physiological imbalances that are identifiable and addressable.
PMS and PMDD sit on the same spectrum but differ in severity. Premenstrual Dysphoric Disorder is a more severe form where mood-related symptoms are significantly debilitating, interfering with work, relationships, and daily function. Both share the same root causes such as progesterone deficiency, oestrogen dominance, serotonin disruption, and gut-brain axis dysfunction but PMDD represents a more pronounced physiological sensitivity to the hormonal shifts of the luteal phase. The functional approach addresses both through the same root cause framework.
PMS has become increasingly common in Indian women driven by diets high in refined carbohydrates that dysregulate blood sugar and worsen hormonal fluctuations, chronic psychological stress that elevates cortisol and suppresses progesterone, widespread magnesium and B6 deficiency that directly impairs the serotonin synthesis needed for mood stability, gut dysbiosis that impairs oestrogen metabolism and clearance, and sedentary lifestyles that reduce the body's ability to regulate inflammation across the cycle. What is dismissed as normal monthly suffering is almost always a measurable physiological pattern.
In most cases of PMS, the central driver is a relative imbalance between oestrogen and progesterone in the luteal phase where oestrogen remains elevated while progesterone fails to rise adequately. This imbalance directly disrupts serotonin, GABA, and dopamine signalling which is why PMS feels so strongly emotional and neurological. The gut plays a critical role here: a dysbiotic microbiome impairs oestrogen clearance, keeping oestrogen elevated and worsening the imbalance. Address progesterone support, oestrogen metabolism, and gut health together and PMS often resolves significantly within one to two cycles.
The Difference Between Managing PMS and Reversing It
CONVENTIONAL MEDICINE
- Oral contraceptive pill to suppress the natural hormonal cycle
- Antidepressants like SSRIs are prescribed for mood-related symptoms
- Pain relief for physical symptoms
- Advice to exercise and reduce stress
- No investigation into why the luteal phase hormonal transition is dysregulated
FUNCTIONAL NUTRITION
- Root Cause Analysis with 60+ Functional Markers
- Luteal phase progesterone, oestrogen, and oestrogen metabolite ratios
- Gut health markers, inflammatory indicators, cortisol rhythm
- Magnesium, B6, zinc, iron, and Vitamin D status
- A dedicated functional nutritionist guides every step
PMS Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as PMS Doesn't End There
77% of clients reported significant reduction in mood-related and physical PMS symptoms within the first two cycles of their personalised protocol.
How We Find and Fix the Root Cause of ED









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of ED

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
No. The pill suppresses your natural hormonal cycle entirely including the luteal phase fluctuations that drive PMS. When you stop it, the underlying imbalances return, often more pronounced. The pill is a temporary override, not a solution.
For most women, significant reversal is entirely achievable. When the root causes like low progesterone, oestrogen dominance, gut dysfunction, and nutrient deficiencies are identified and addressed, PMS symptoms reduce substantially within one to three cycles. Many of our clients experience their first symptom-free luteal phase within 60 days of beginning their protocol.
Completely. The emotional symptoms of PMS are directly driven by how hormonal fluctuations in the luteal phase affect serotonin, GABA, and dopamine, the neurotransmitters governing mood and anxiety. Low progesterone reduces GABA activity, producing anxiety. Oestrogen dominance disrupts serotonin synthesis. Magnesium and B6 deficiency impair the production of both. These are measurable physiological processes, not psychological weakness.
PMDD sits at the severe end of the same hormonal spectrum as PMS, with more pronounced neurological sensitivity to luteal phase hormonal shifts. The root causes are the same and the functional approach addresses both. PMDD typically requires a more targeted and sustained protocol, but significant improvement is consistently achievable and complete resolution is possible for many women.
Most clients notice measurable improvement within the first one to two cycles of beginning their personalised protocol particularly in mood stability, bloating, and energy. Deeper hormonal rebalancing, including consistent progesterone normalisation and oestrogen clearance, typically consolidates over three to four months of sustained intervention.






Talk to our team

Talk to our team
Download Now
