Heavy Metals Accumulate Silently for Years. By the Time You Feel Them, They've Already Been Disrupting Your Biology for a Long Time.
Book Your Root Cause Analysis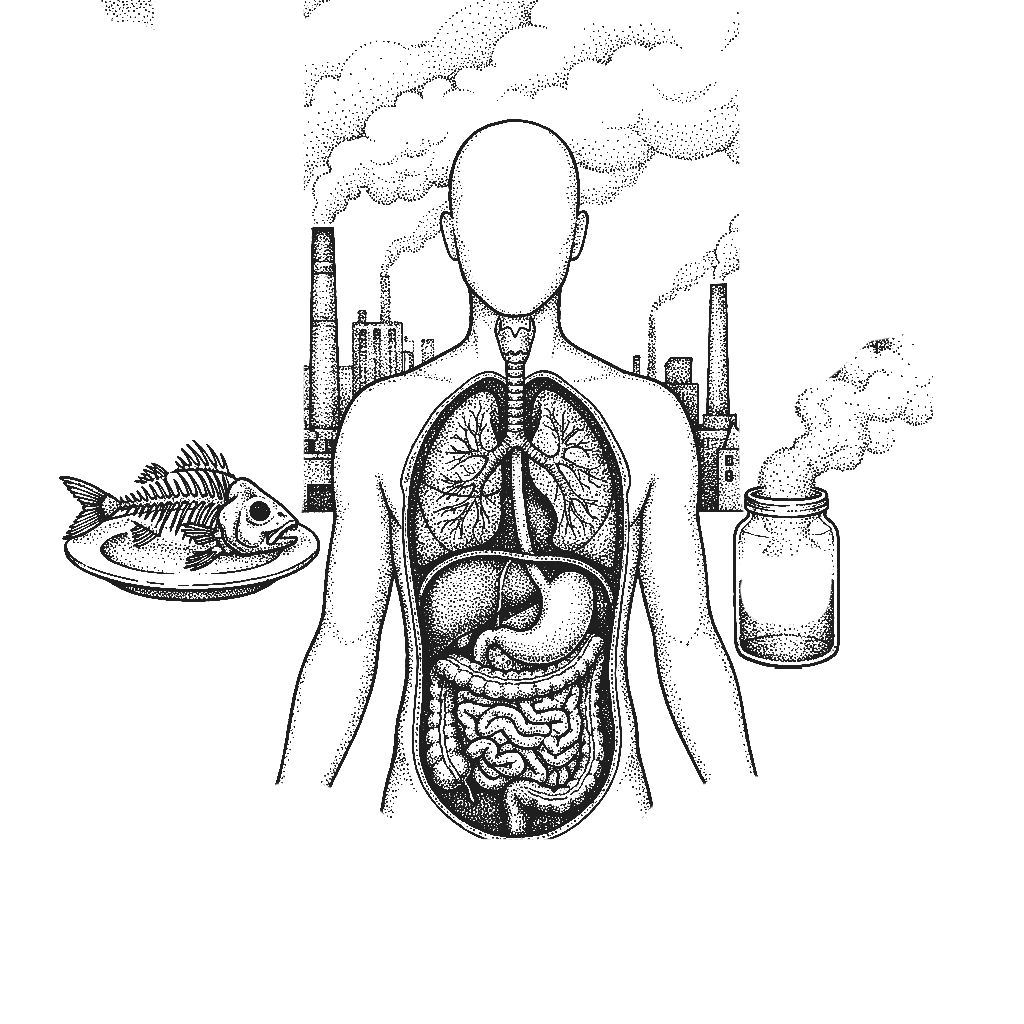
If You See Yourself Here, Don't Ignore It










Heavy Metal Toxicity Isn't Rare. It's Rarely Tested For.

Heavy metal burden refers to the accumulation of toxic metals including lead, mercury, arsenic, cadmium, and aluminium in the body's tissues, organs, and bones over time. Unlike acute poisoning, which is dramatic and immediately recognisable, chronic low-level accumulation is subtle and progressive. These metals interfere with enzymatic processes, disrupt hormonal signalling, damage mitochondrial function, impair detoxification pathways, and drive chronic inflammation. Because their effects are systemic and non-specific, they produce a symptom picture that overlaps with dozens of other conditions and is almost never attributed to its actual source.
Sources are far more common than most people realise. In India specifically: contaminated groundwater and municipal water supplies carrying arsenic and lead, rice and vegetables grown in heavy-metal-rich soil, fish and seafood carrying mercury, cookware and food packaging leaching aluminium and other metals, occupational exposure in manufacturing, construction, and agriculture, air pollution in urban centres, dental amalgam fillings releasing mercury over time, and cosmetic products including skin-lightening creams containing mercury and lead. Exposure is not exceptional. It is routine for a large proportion of the population.
Standard blood panels do not include heavy metal testing. Heavy metals move out of the blood relatively quickly and deposit in tissue and bone, meaning blood levels are normal even when tissue burden is significant. Accurate assessment requires specific urine or hair analysis combined with a clinical picture, neither of which is part of routine medical investigation. Without targeted testing, the burden is invisible to conventional medicine.
Heavy metals do not cause a single identifiable disease. They degrade the terrain, further impairing the detoxification, hormonal, immune, and neurological systems that every other process depends on. Someone with a significant heavy metal burden will present with fatigue, brain fog, hormonal disruption, gut dysfunction, and poor immunity and will be investigated and treated for each of these separately, with limited success, because the common driver has never been identified. Address the metal burden and the downstream dysfunction very often begins to resolve.
Three steps to finally understanding your body
CONVENTIONAL MEDICINE
- No routine heavy metal testing in standard panels
- Symptoms attributed to stress, ageing, or idiopathic causes
- Chelation offered only in cases of acute, severe poisoning
- No assessment of tissue burden, detoxification capacity, or cumulative exposure
- Each downstream symptom managed separately with no connecting investigation
FUNCTIONAL NUTRITION
- Root Cause Analysis with 60+ functional markers
- Specific heavy metal markers including lead, mercury, arsenic, cadmium, and aluminium
- Liver detoxification capacity and phase 1 and 2 pathway function
- Glutathione status and oxidative stress markers
- Gut health, intestinal permeability, and mineral status
- A dedicated functional nutritionist guides every step
Heavy Metal Burden Isn’t One Problem, It’s Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as Accumulation Doesn't End There
69% of clients presenting with chronic multi-system symptoms identified significant heavy metal burden or critically impaired detoxification pathways in their Root Cause Analysis and reported measurable improvement in energy, cognition, and symptom load within 60 days of their personalised protocol.
They felt the same way you do right now.









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find the Toxic Load Nobody Else Has Looked For

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
Yes. The most common sources of heavy metal exposure in India are not industrial, they are dietary and environmental. Contaminated water, rice, fish, cookware, cosmetics, and urban air pollution are sufficient for significant accumulation over years. You do not need occupational exposure to carry a meaningful toxic burden.
Blood testing is not an accurate measure of tissue metal burden. Metals clear from the blood within days and deposit in organs, bones, and fat tissue. Accurate assessment requires specific urine or hair analysis alongside a functional marker panel neither of which is included in standard blood work.
When done correctly and supported nutritionally, yes. Aggressive chelation without supporting detoxification pathways and mineral status can cause harm which is why a structured, targeted approach based on your specific markers is essential. The goal is effective clearance without overwhelming the system.
Directly. Heavy metals are endocrine disruptors, they interfere with oestrogen, testosterone, thyroid hormones, and adrenal function. This is why hormonal symptoms including irregular cycles, low testosterone, and thyroid dysfunction are common in people with unidentified metal burden.
It depends on the metals involved, the duration and level of exposure, and the integrity of your detoxification pathways. Meaningful improvement in symptoms typically begins within 60 to 90 days of a targeted protocol. Full clearance of deep tissue burden takes longer and is assessed through repeat testing over time.






Talk to our team

Talk to our team
Download Now
