Atherosclerosis Begins Decades Before a Heart Attack. Most People Have No Idea It Is Already Progressing.
Book Your Root Cause Analysis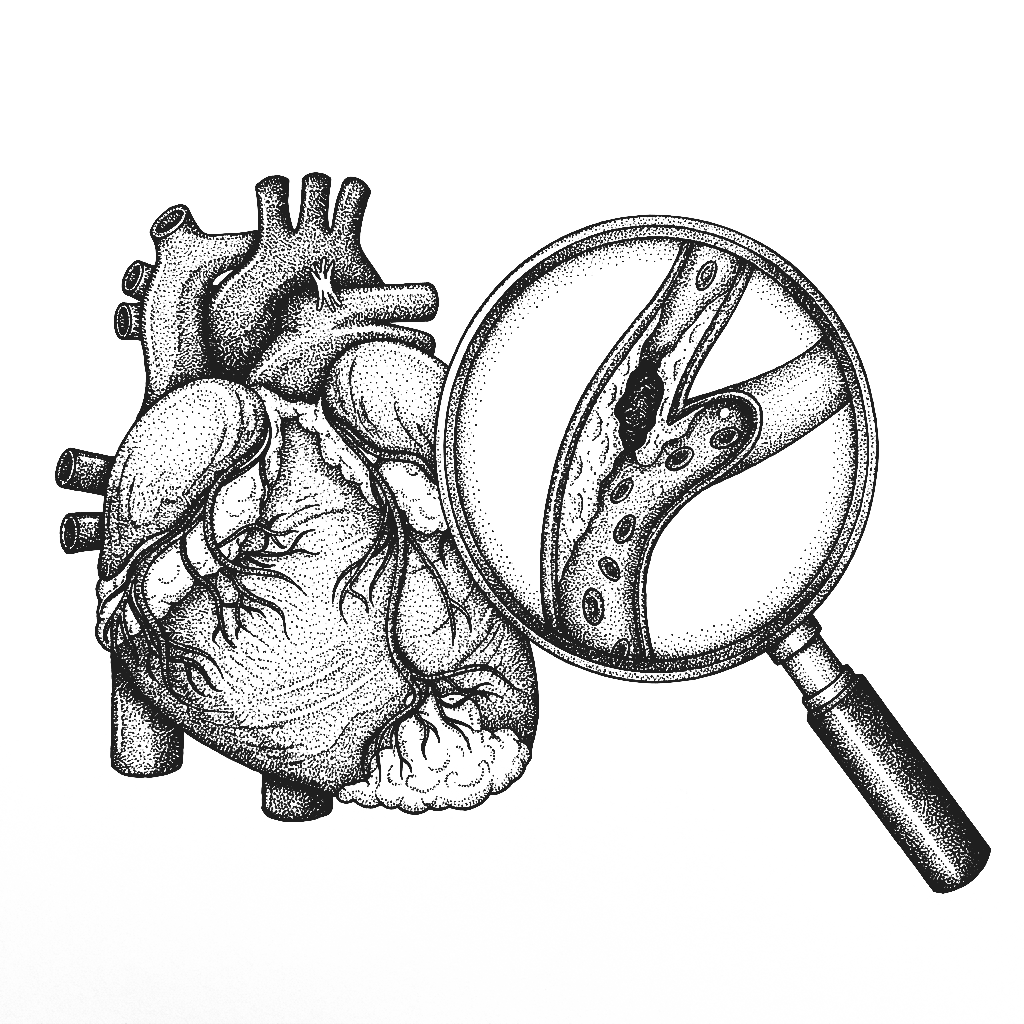
Atherosclerosis Isn't What You Think It Is












Atherosclerosis Isn't What You Think It Is

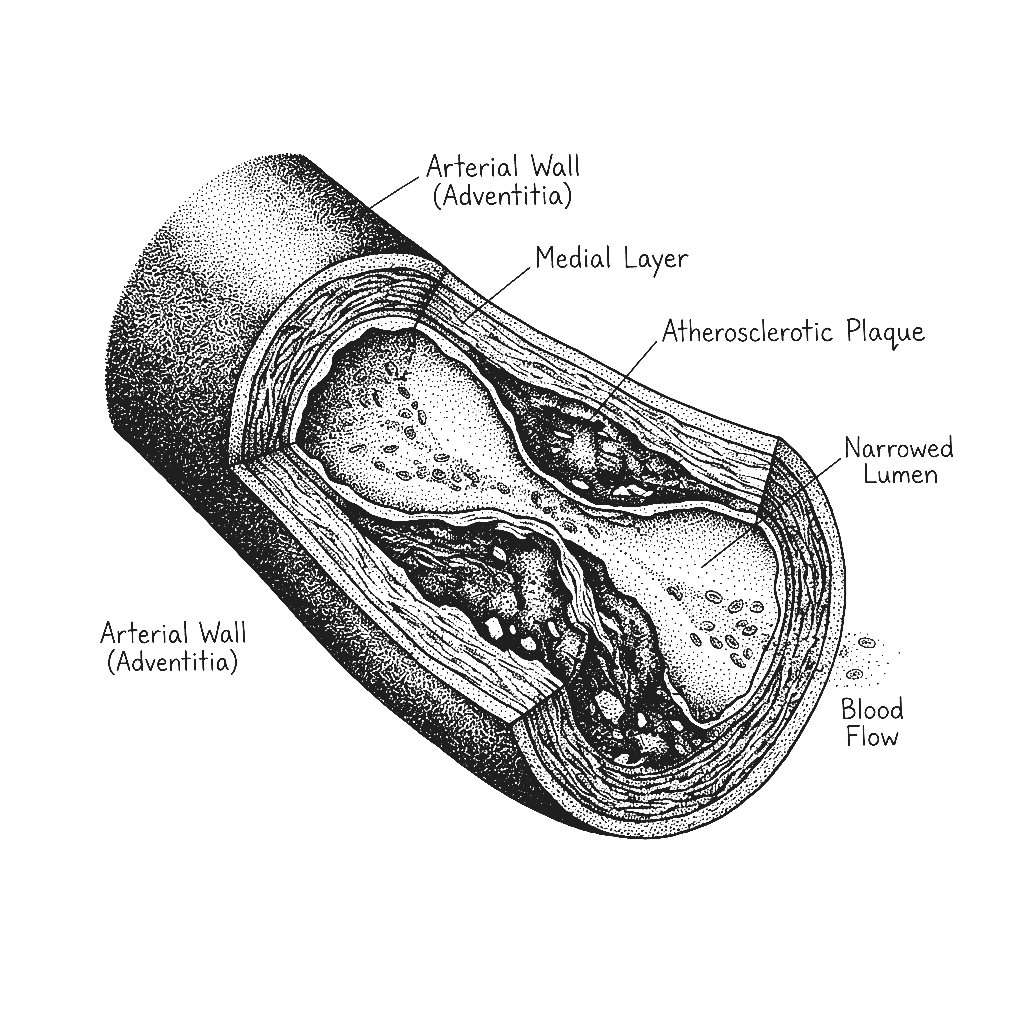
Atherosclerosis is the progressive buildup of plaques composed of oxidised lipids, immune cells, calcium, and fibrous tissue within the walls of arteries. It is the underlying structural disease behind the majority of heart attacks, strokes, and peripheral arterial disease. Atherosclerosis is not simply a consequence of high cholesterol or a fatty diet. It is an inflammatory disease of the arterial wall initiated by endothelial dysfunction, driven by oxidative stress and immune activation, and accelerated by insulin resistance, chronic inflammation, and metabolic dysfunction. Cholesterol is involved but it is a passenger in a process driven by inflammation, and not the primary cause. This distinction is critical because it determines what needs to be addressed to actually halt and reverse the process.
The process begins with endothelial dysfunction damage to the single cell layer lining the inside of arterial walls that is responsible for producing nitric oxide, regulating vascular tone, and maintaining a barrier against lipid infiltration. When this lining is damaged by oxidative stress, chronic inflammation, elevated insulin, smoking, or mechanical stress from hypertension such as LDL particles, particularly small dense oxidised ones, infiltrate the arterial wall. The immune system mounts a response sending macrophages to engulf the oxidised LDL. These macrophages become foam cells and accumulate forming fatty streaks that progressively enlarge into plaques. Over decades these plaques grow, calcify, and narrow the arterial lumen until a plaque ruptures triggering a clot that causes a heart attack or stroke.
Fatty streaks, the earliest stage of atherosclerosis, have been found in the arteries of teenagers and young adults in autopsy studies. The process begins decades before symptoms appear and decades before any conventional cardiovascular risk assessment would trigger concern. The metabolic and inflammatory drivers including insulin resistance, endothelial dysfunction, oxidative stress, chronic inflammation begin operating in early adulthood and accumulate silently. By the time a person is told their cholesterol or blood pressure is concerning, arterial damage has typically been building for twenty to thirty years.
Indians develop atherosclerosis and cardiovascular disease at younger ages, lower cholesterol levels, and lower body weights than Western populations. The genetic predisposition toward insulin resistance and atherogenic dyslipidaemia such as high triglycerides, low HDL, and small dense LDL combined with the rapid dietary transition toward refined carbohydrates, chronic psychological stress, widespread vitamin D deficiency, sedentary urban lifestyles, and high rates of metabolic syndrome create conditions in which atherosclerosis progresses faster and more severely than standard risk models predict. India has one of the highest rates of premature cardiovascular disease in the world and the majority of it traces back to addressable metabolic and inflammatory drivers.
Atherosclerosis is managed as a cholesterol problem requiring lipid lowering medication. What it actually is is an inflammatory disease of the arterial wall driven by endothelial dysfunction, oxidative stress, insulin resistance, and chronic immune activation with cholesterol as one participant in a much more complex process. Statins reduce LDL and have modest anti-inflammatory effects. They do not restore endothelial function, do not correct insulin resistance, do not address oxidative stress, and do not resolve the chronic inflammation driving plaque progression. Address those drivers and atherosclerotic progression slows, stabilises, and in many cases partially reverses as demonstrated in well-conducted clinical trials of comprehensive lifestyle and nutritional intervention.
The Difference Between Managing Atherosclerosis and Addressing Its Drivers
CONVENTIONAL MEDICINE
- Standard lipid panel and cardiovascular risk score calculation
- Statins as primary intervention for elevated LDL
- Antihypertensives for blood pressure management
- Aspirin for secondary prevention
- Advice to reduce dietary fat, exercise, and stop smoking
- No assessment of endothelial function, oxidative stress, or insulin resistance
FUNCTIONAL NUTRITION
- Root Cause Analysis with 60+ functional markers
- Advanced lipid panel including LDL particle size, oxidised LDL, and Lp(a)
- Inflammatory markers including hsCRP, homocysteine, and fibrinogen
- Fasting insulin, HOMA-IR, and full glucose metabolism panel
- Endothelial function markers and oxidative stress indicators
- Vitamin D, magnesium, CoQ10, and omega 3 status
- A dedicated functional nutritionist guides every step
Atherosclerosis Isn't One Problem. It's Multiple Root Causes Working Together.

Three steps to finally understanding your body

Book your Root Cause Analysis

Get your blood work done at Home

Sit down with your nutritionist
What Starts as Atherosclerosis Doesn't End There

71% of clients with confirmed cardiovascular risk and atherosclerotic markers reported measurable improvement in inflammatory markers, lipid pattern, and endothelial function indicators within the first 60 days of their personalised protocol.
They felt the same way you do right now.









.png)





Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
Before
After
How We Find and Fix the Root Cause of Atherosclerosis

Personalised Diet Protocol

Smart Supplementation

Lifestyle Interventions
FAQs
Statins reduce LDL and have modest anti-inflammatory effects that provide cardiovascular benefit in high risk populations. But LDL in isolation is a poor predictor of atherosclerotic risk and statins do not address endothelial dysfunction, insulin resistance, oxidative stress, or the inflammatory burden driving plaque progression. Many people develop heart attacks with normal LDL levels. The complete picture requires a comprehensive assessment of the actual drivers, not a single number.
Plaque regression, an actual reduction in plaque volume has been demonstrated in clinical trials of comprehensive lifestyle and nutritional intervention. The most well known is the Ornish programme but subsequent research has shown that multiple targeted interventions addressing inflammation, oxidative stress, and metabolic dysfunction can produce measurable plaque regression assessed by imaging. Halting progression and stabilising vulnerable plaques is achievable in virtually all cases when the root causes are addressed.
Lp(a) is largely genetically determined and cannot be meaningfully reduced by dietary or lifestyle intervention alone. However elevated Lp(a) increases cardiovascular risk only in the context of a pro-inflammatory, oxidative, and metabolically dysfunctional environment. Addressing all other modifiable risk factors such as inflammation, insulin resistance, endothelial function, oxidative stress substantially reduces the cardiovascular impact of elevated Lp(a) even when Lp(a) itself cannot be lowered.
This is one of the most important connections in cardiovascular medicine. Insulin resistance drives endothelial dysfunction, promotes small dense LDL production, elevates triglycerides, lowers HDL, increases arterial wall inflammation, and impairs the body's ability to repair arterial damage. People with insulin resistance have dramatically elevated atherosclerotic risk even at normal LDL levels. Correcting insulin resistance is one of the most impactful cardiovascular interventions available.
Yes and this is particularly important for secondary prevention. The majority of people who have experienced a cardiac event have the same unaddressed metabolic and inflammatory drivers that caused the first event continuing to drive progression. Functional nutrition works alongside cardiac rehabilitation and medical management to address those drivers, further reducing the risk of a second event in a way that medication alone cannot fully achieve.






Talk to our team

Talk to our team
Download Now
