.svg)
.svg)







Introduction
Picture a 28 year old woman in India. Her periods have been irregular for over a year. She has been told she probably has PCOS. Her thyroid panel came back normal. She has been put on birth control to regulate her cycle, but the moment she stops, the irregularity returns. Nobody has checked her prolactin yet.
This is not a rare story. Research shows that between 25 and 37% of women presenting with unexplained infertility have elevated prolactin levels, yet a prolactin test is still not universally included in early hormonal workups.
Hyperprolactinemia, chronically elevated prolactin, is one of the most underdiagnosed hormonal disruptions in women of reproductive age. It derails periods, blocks ovulation, feeds mood instability, and creates a confusing symptom picture that points in every direction except the right one.
How Common Is This? The Numbers That Should Alarm Us
Before diving into symptoms, it is worth pausing on how widespread this condition actually is in India.
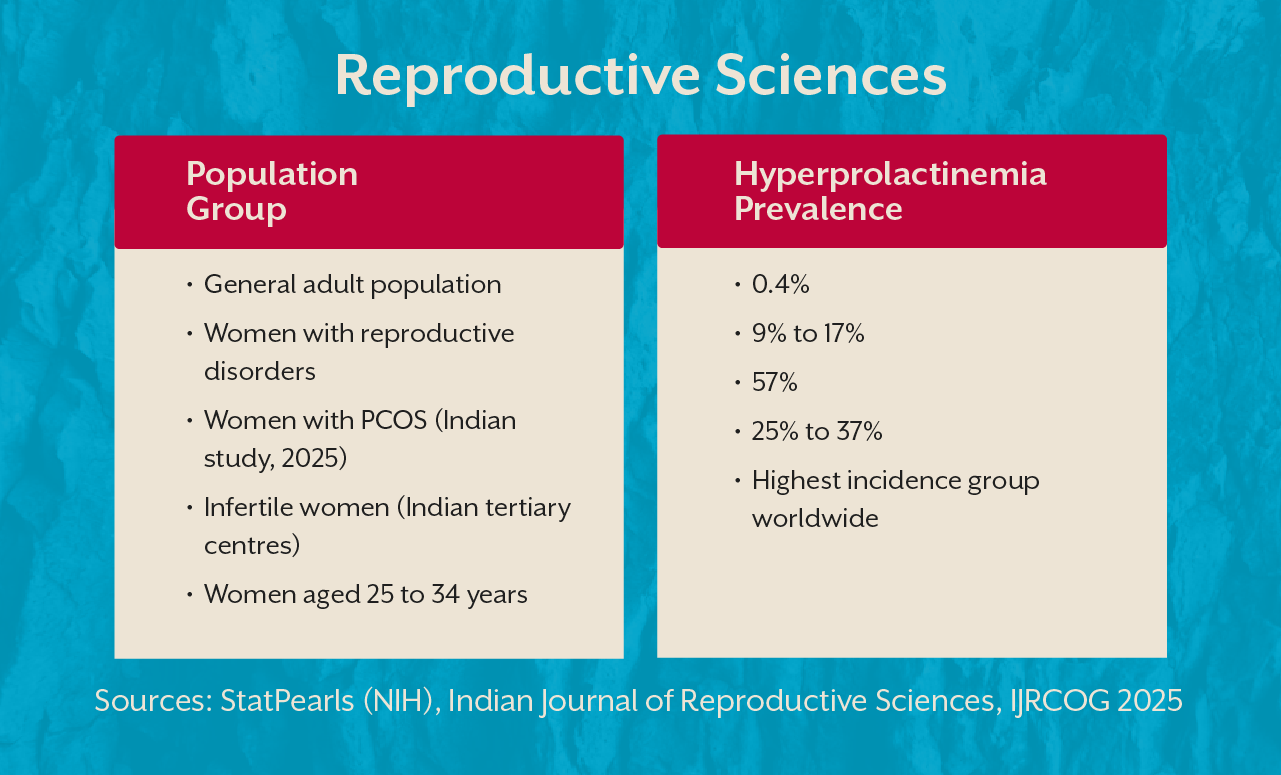
That last row is particularly striking. In a 2025 Indian study of 110 women with PCOS, over half had hyperprolactinemia. These are not numbers from a rare endocrine condition. They are the everyday hormonal reality of Indian women.
What Is Hyperprolactinemia and Why Does It Hit Women Hardest
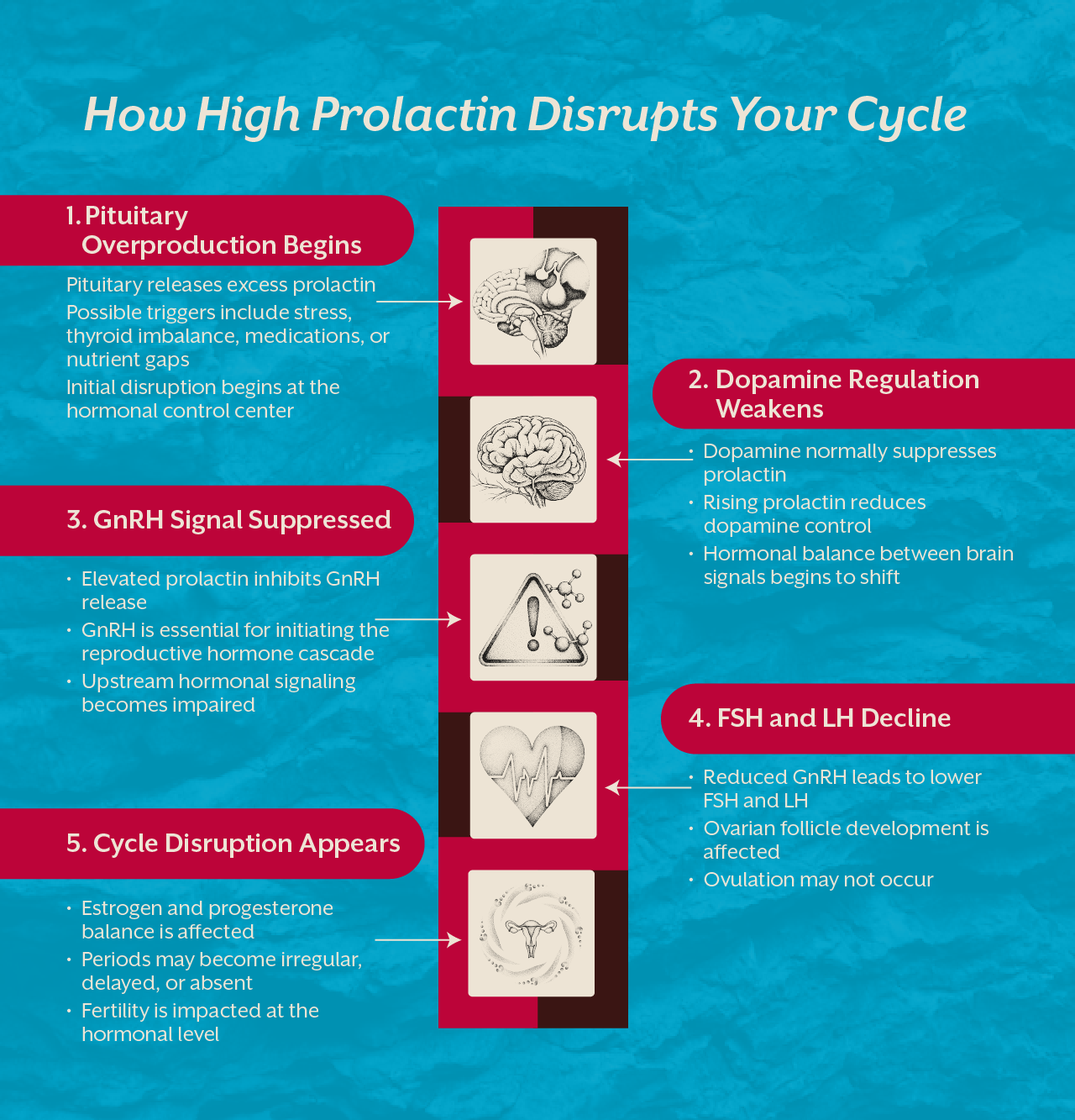
Prolactin is a hormone made by the pituitary gland. Its primary role is to trigger breast milk production after childbirth. Outside of pregnancy and nursing, prolactin should stay low. When it rises without a biological reason, the consequences are significant because prolactin directly suppresses FSH and LH, the two hormones that govern the menstrual cycle.
When prolactin climbs, FSH and LH fall. When FSH and LH fall, ovulation stops. And when ovulation stops, the period disappears or grows erratic. This is the central mechanism driving hyperprolactinemia symptoms in females, and why the period is always the first thing to go.
Women carry a far greater burden of this condition than men. The female hormonal system is simply more sensitive to prolactin fluctuations because the reproductive cycle depends on getting it right.
Hyperprolactinemia Causes: What Is Actually Driving Your Prolactin Up
The cause is not always the same and treatment depends entirely on finding the right driver.
Prolactinoma
The most common structural cause is a prolactinoma, a benign pituitary tumour that overproduces prolactin. These account for nearly half of all pathological cases and are more common in women than men. Women typically develop smaller microprolactinomas that are harder to detect on routine imaging, which is one reason diagnosis is so often delayed.
Hypothyroidism
When the thyroid is underactive, excess TRH directly stimulates prolactin secretion. A woman with poorly managed hypothyroidism may have elevated prolactin purely as a downstream consequence. Treating the thyroid often normalises prolactin entirely, without any direct prolactin intervention at all.
Medications
Antipsychotics, certain antidepressants, blood pressure medications, and antiemetics raise prolactin by blocking dopamine, the brain chemical that normally keeps prolactin suppressed. This dopamine connection is central to understanding the condition and why nutritional support can genuinely make a difference.
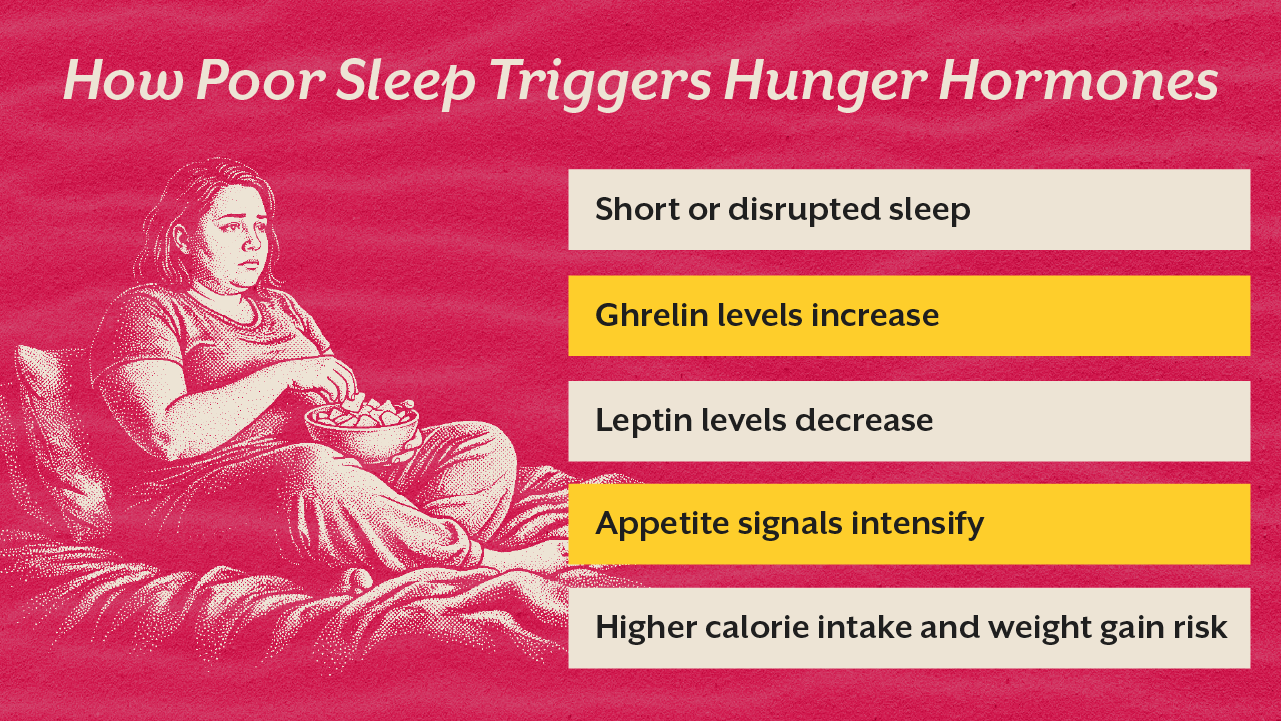
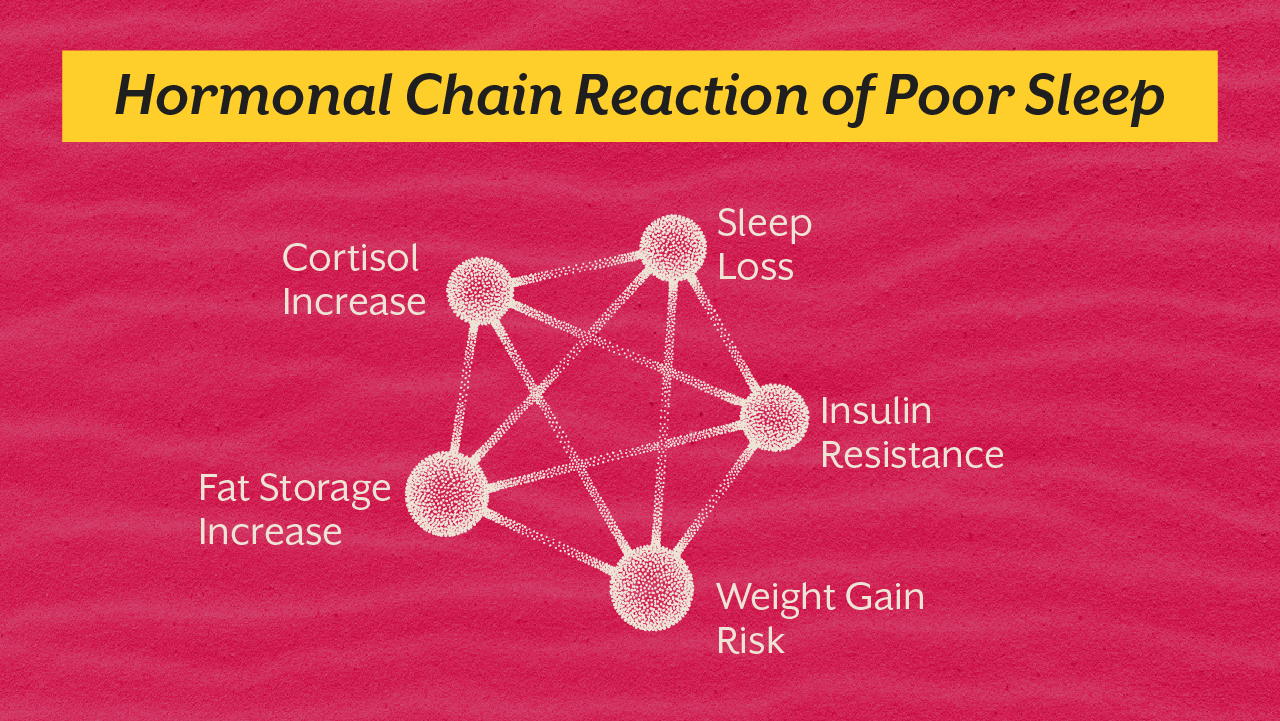
Chronic Stress and Sleep Disruption
Prolactin rises with physical stress, poor sleep, and sustained high cortisol. Women who are consistently overworked and under-rested often carry mild to moderate prolactin elevation that nobody connects to their symptoms. The overlap with burnout is real. Read our blog on Addison's Disease Symptoms in Women Mistaken for Burnout for a fuller picture of how stress-related hormonal conditions disguise themselves.

Hyperprolactinemia Symptoms in Females: What Your Body Is Saying
Prolactin and Irregular Periods
The relationship between prolactin and irregular periods is direct. Elevated prolactin suppresses GnRH, which reduces FSH and LH from the pituitary. Without these signals, the ovaries do not ovulate. Periods arrive late, become very light, or stop entirely. The cycle irregularity is the symptom. Elevated prolactin is the cause.
Galactorrhea: Milk Without Pregnancy
One of the more startling high prolactin symptoms in women is galactorrhea, the spontaneous production of breast milk in a woman who is not pregnant or breastfeeding. This occurs in roughly one third to half of women with hyperprolactinemia. Many women notice it and stay silent, assuming it is normal. It is not. It is a direct sign that prolactin is biologically elevated and active.
Prolactin Fertility Problems
Elevated prolactin blocks ovulation and therefore blocks conception. Women who have been trying to conceive for over a year with irregular cycles should have prolactin tested as a first-line investigation. In Indian infertility studies, elevated prolactin was found in nearly 37% of women with endocrine-related infertility. Prolactin fertility interference is one of the most treatable causes of anovulatory infertility once properly identified.
Mood Shifts, Low Libido, and Brain Fog
Elevated prolactin suppresses estrogen, and low estrogen drives depression, poor libido, brain fog, and emotional flatness. Women describe a version of themselves they do not recognise: disinterested, flat, and disconnected. These are biological symptoms, not character changes. Some are placed on antidepressants that raise prolactin further, quietly worsening the very hormonal environment they are trying to correct.
The Dopamine Connection: Why This Is a Brain Chemistry Problem Too
Prolactin secretion is controlled primarily by dopamine, which is released continuously from the hypothalamus. Dopamine truly suppresses prolactin. When dopamine falls, prolactin rises promptly. This is not just pharmacology, rather it is nutritional biochemistry.
Dopamine synthesis requires tyrosine, vitamin B6, iron, and zinc. When a woman is chronically stressed, nutritionally depleted, or sleeping poorly, dopamine production suffers and prolactin climbs. Lifestyle and nutrition are not optional extras here. They sit directly at the root of the mechanism.
Think of dopamine as the valve and the prolactin as the water. When the valve is strong enough, the water stays controlled. When it weakens, everything overflows.
Hyperprolactinemia Natural Treatment: The Nutritional Foundation
Medical treatment through dopamine agonists is the clinical standard for prolactinomas. But for women with idiopathic or mildly elevated prolactin, targeted nutritional support can produce meaningful change. Hyperprolactinemia natural treatment is not a replacement for medical investigation. It is the biological foundation that makes any treatment more effective.
Vitamin B6
Vitamin B6 is a critical cofactor in dopamine synthesis. Studies have shown that B6 supplementation can minimise elevated prolactin in women with idiopathic hyperprolactinemia. Without adequate B6, the enzymatic step that converts tyrosine into dopamine cannot complete efficiently, and prolactin suppression weakens over time.
Zinc
Zinc plays a direct role in regulating pituitary function as well as prolactin release. Zinc deficiency impairs dopamine receptor sensitivity and has been linked to elevated prolactin. Women experiencing hair thinning or acne alongside cycle irregularity should have zinc status assessed as part of their hormonal investigation.
Hyperprolactinemia Diet: What to Build Your Plate Around
A hyperprolactinemia diet is a rebuilding plan, not a restriction list. Prioritise tyrosine-rich foods: eggs, chicken, nuts, and seeds. Add magnesium-rich foods like pumpkin seeds for dopamine receptor support. Include vitamin C rich fruits and vegetables to reduce oxidative stress at the pituitary level. Stable blood sugar is non-negotiable since cortisol spikes directly drive prolactin upward. Avoid alcohol, excessive caffeine, and ultra-processed foods that disrupt hypothalamic signalling.
What Actually Confirms Hyperprolactinemia
Diagnosis begins with a fasting morning serum prolactin test, drawn at least 2 hours after waking and before any physical exertion. A single elevated reading is not sufficient for diagnosis. A second confirmatory test is needed before any treatment decision is made.
If prolactin remains elevated, a pituitary MRI is ordered to check for adenoma. Thyroid function and medication history are reviewed simultaneously. Finding the root cause, rather than simply suppressing the number, determines whether treatment will hold.
If you are experiencing irregular periods, unexplained infertility, or mood disruption alongside cycle changes, a root cause analysis can map the full hormonal picture rather than treating each symptom in isolation.
Key Takeaway
Hyperprolactinemia is not rare. It is one of the most common hormonal conditions in Indian women of reproductive age, hiding behind missed periods, unexplained infertility, and mood changes written off as stress for years.
A single prolactin blood test can begin to change an entire diagnostic story. Whether the driver is a pituitary adenoma, an underactive thyroid, B6 and zinc deficiency, or chronic dopamine depletion, this condition has clear mechanisms and clear pathways of support. It goes undertreated not because it is complex, but because it goes untested.
If your hormonal picture feels incomplete and the standard answers are not adding up, do not wait. Book a consult and let the right investigation finally begin.