
.svg)
.svg)







Introduction
Erectile dysfunction is often discussed in whispers. Many men experience it. Few talk about it openly. A weak erection, reduced stamina, or declining sexual drive is commonly attributed to age, stress, or performance anxiety. Medication is often prescribed quickly. Yet what if impotence is not primarily a performance problem but a cellular energy problem?
At iThrive Alive, we view erectile dysfunction as a vascular and metabolic signal. An erection is not simply a mechanical event. It is a complex neurovascular response that depends on nitric oxide release, endothelial integrity, mitochondrial ATP production, and balanced hormonal signaling. When these systems are impaired, dysfunction appears.
Before labeling it psychological or inevitable, it is important to ask a deeper question. Is your body metabolically capable of sustaining optimal blood flow and cellular energy? Because in many men, the real cause of ED lies in mitochondrial dysfunction long before cardiovascular disease becomes visible.
The Biology of an Erection and Why Energy Matters
An erection requires coordinated communication between the brain, nerves, blood vessels, and smooth muscle tissue. Sexual stimulation triggers nitric oxide release from endothelial cells lining penile arteries. Nitric oxide activates cyclic GMP pathways, relaxing smooth muscle and allowing increased blood flow into the corpus cavernosum.
This process is energy dependent. Nitric oxide synthesis requires functional endothelial cells. Endothelial cells rely heavily on mitochondria for ATP production. If mitochondrial efficiency declines, nitric oxide signaling weakens. Blood flow becomes compromised. The erection is softer or unsustained.
Mitochondrial dysfunction also increases oxidative stress. Reactive oxygen species degrade nitric oxide and damage vascular lining. Over time, this reduces vascular elasticity and responsiveness.
This is why erectile dysfunction is sometimes described as an early warning sign of cardiovascular dysfunction. The penile arteries are smaller than coronary arteries. They show dysfunction earlier.
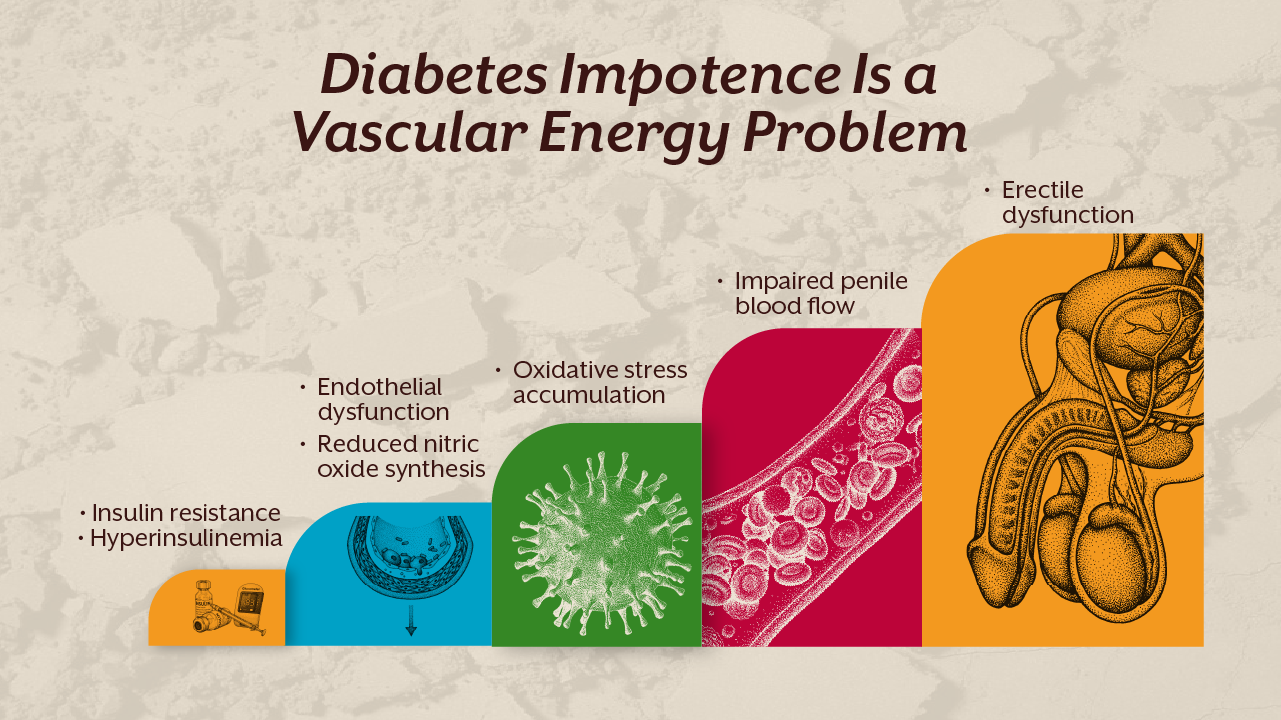
The Metabolic Link Between Diabetes and Impotence
One of the strongest associations with erectile dysfunction is diabetes. In fact, diabetes impotence is not rare. Chronic hyperglycemia damages endothelial cells through advanced glycation end products. These compounds impair nitric oxide synthesis and increase oxidative stress.
But the process starts earlier than diabetes diagnosis. As discussed in our blog “Insulin Resistance: The Silent Phase Before Type 2 Diabetes”, insulin resistance precedes overt hyperglycemia by years. Elevated insulin levels impair endothelial function even before glucose rises significantly.
Hyperinsulinemia reduces nitric oxide availability. It also promotes inflammation and vascular stiffness. Over time, microvascular circulation declines. Erectile dysfunction becomes one of the earliest visible manifestations of metabolic syndrome.
Mitochondria are particularly sensitive to glucose variability. Frequent spikes in blood sugar increase reactive oxygen species production inside mitochondria. This further damages endothelial cells.
If the cause of ED is metabolic, then addressing insulin resistance is not optional. It is foundational.
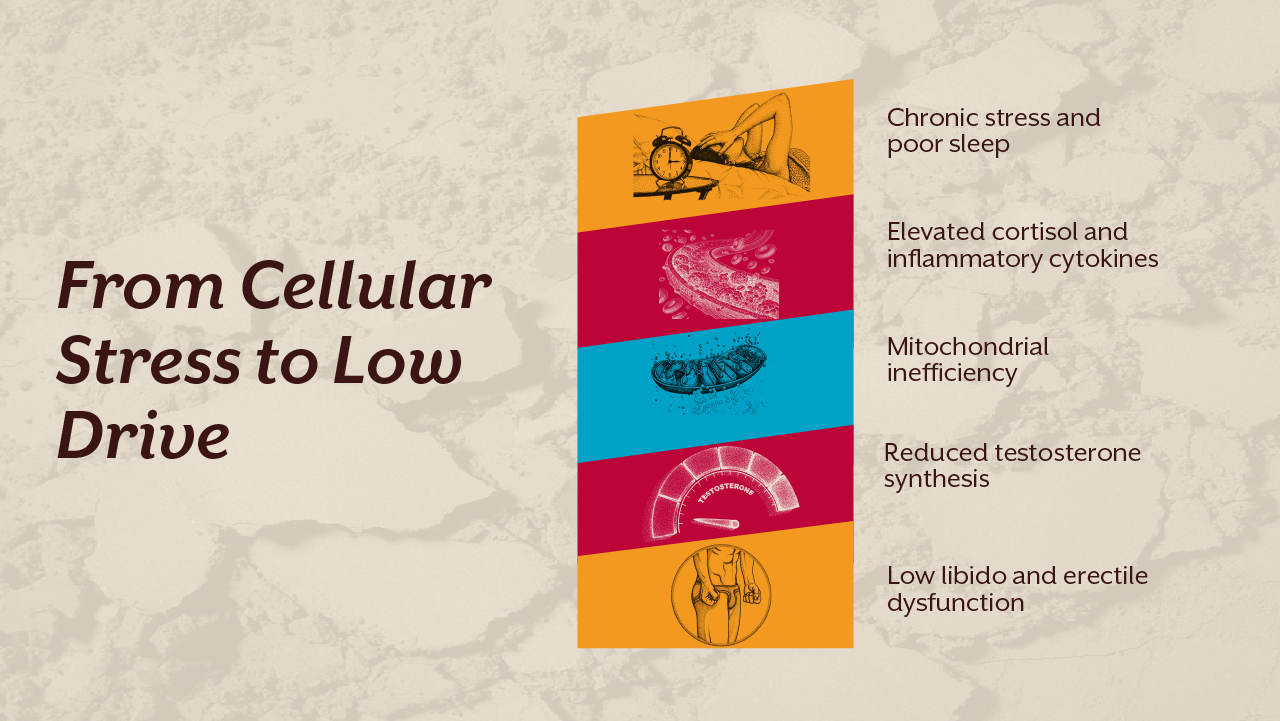
Testosterone, Mitochondria, and Libido
Low drive is often blamed on low testosterone. While hormonal decline can contribute, testosterone production itself is mitochondria dependent. The first step of steroidogenesis occurs in the mitochondria of Leydig cells. Cholesterol conversion to pregnenolone requires mitochondrial enzymes and adequate ATP.
Chronic metabolic stress impairs this pathway. Inflammatory cytokines suppress hypothalamic signaling. Sleep deprivation reduces luteinizing hormone pulses. Micronutrient deficiencies such as zinc and magnesium impair enzymatic reactions involved in testosterone synthesis.
Therefore, libido decline is not only a hormonal issue. It is a metabolic resilience issue.
In our clinical framework at iThrive Alive, hormonal evaluation is integrated with metabolic assessment. We do not treat numbers in isolation. We assess insulin markers, inflammatory load, nutrient sufficiency, thyroid balance, and stress physiology before concluding that testosterone replacement is necessary.
What You Can Do If the Cause of ED Is Metabolic
If erectile dysfunction is rooted in mitochondrial dysfunction, the strategy must address cellular energy.
First, stabilize glucose variability. Smart eating types that reduce post meal spikes support mitochondrial integrity. Protein anchored meals improve satiety and reduce insulin surges. This approach aligns with principles outlined in our case study “Targeted Nutritional Intervention in PCOS Associated Metabolic Dysfunction A Root Cause Analysis and Functional Nutrition driven Case Study”, where metabolic correction restored hormonal rhythm.
Second, incorporate structured resistance training. Skeletal muscle acts as a glucose sink. Improving GLUT4 translocation enhances insulin sensitivity independent of insulin levels. Better insulin sensitivity reduces endothelial stress.
Third, prioritize micronutrient sufficiency. Magnesium supports ATP production. Zinc supports testosterone synthesis. Selenium influences thyroid mediated metabolic rate. CoQ10 supports mitochondrial electron transport chain efficiency. Supplementation should be individualized based on assessment.
Fourth, regulate sleep and circadian rhythm. Testosterone peaks during deep sleep. Mitochondrial repair processes are circadian regulated. Chronic sleep deprivation perpetuates dysfunction.
Fifth, evaluate inflammatory markers and gut health where indicated. Chronic systemic inflammation impairs vascular elasticity.
This is where a structured evaluation becomes valuable. Instead of guessing the cause of ED, men can book a root cause analysis to identify whether insulin resistance, micronutrient depletion, or inflammatory stress is the dominant driver. If you are unsure where to begin, you can book a consult to understand your metabolic landscape.

A Systems Approach to Erectile Dysfunction
Erectile dysfunction is rarely isolated. It is often an early vascular alarm. The same metabolic pathways that lead to diabetes and cardiovascular disease influence penile blood flow. Addressing dysfunction at the mitochondrial and endothelial level offers broader protection.
Medication may improve short term blood flow. But without improving cellular energy and metabolic signaling, the underlying cause remains active.
At iThrive Alive, we focus on lifestyle intervention, smart supplementation, and precision nutrition because vascular health reflects metabolic health. When mitochondria function efficiently, endothelial cells respond effectively, hormonal rhythm stabilizes, and performance improves organically.
Key Takeaway
If you are experiencing weak erection or low drive, understand that your body may be signaling metabolic stress rather than failure. Erectile dysfunction and impotence are often early indicators of mitochondrial inefficiency, insulin resistance, and endothelial dysfunction. By restoring glucose stability, improving insulin sensitivity, supporting micronutrient status, and optimizing sleep and stress physiology, you address the biological root rather than masking the symptom. Sustainable recovery lies in cellular repair, not temporary stimulation.