.svg)
.svg)







Introduction
If you have been diagnosed with PCOS or polycystic ovary syndrome and are trying to conceive, the experience can feel confusing and emotionally exhausting. You may have been told that ovulation is irregular, that your hormones are imbalanced, or that you might need assisted reproductive procedures. What is often not explained clearly is why PCOS affects fertility in the first place and what you can actually do to improve your chances of pregnancy.
At iThrive Alive, we view PCOS not as a reproductive disorder alone, but as a systemic metabolic and inflammatory condition that alters ovarian signaling. PCOS pregnancy challenges are rarely about the ovaries in isolation. They are usually about insulin resistance, mitochondrial dysfunction, chronic inflammation, micronutrient depletion, and stress physiology altering how the ovaries respond to hormonal signals.
The good news is this. When the internal environment improves, ovulation improves. When metabolic signaling improves, fertility improves. And when root causes are addressed, the need for aggressive interventions often reduces.
Let us understand how.
Why PCOS Affects Fertility Beyond the Ovaries
PCOS fertility treatment is often approached as an ovulation problem. However, ovulation is only the final event in a long cascade of metabolic and hormonal signaling. In polycystic ovary syndrome, the disruption begins much earlier.
Insulin resistance plays a central role. Elevated insulin levels stimulate ovarian theca cells to produce excess androgens. These androgens interfere with follicular maturation. Instead of one dominant follicle maturing and releasing an egg, multiple immature follicles remain arrested. This is why ultrasound often shows a polycystic pattern.
Mitochondrial dysfunction adds another layer. The oocyte is one of the most energy demanding cells in the human body. If cellular energy production is compromised due to oxidative stress or micronutrient insufficiency, egg quality declines even if ovulation is induced.
Chronic inflammation further disrupts hormone receptor sensitivity. Even when hormone levels appear within reference range, cellular responsiveness may be impaired.
This is why standard reports may look acceptable, yet conception does not occur.
The Metabolic Drivers That Delay Conception
Most women with PCOS are advised to lose weight. While weight management can help, focusing only on the scale misses deeper metabolic drivers.
Insulin resistance increases circulating insulin even before blood glucose rises. Hyperinsulinemia worsens androgen excess and impairs ovulatory rhythm. This metabolic pattern is similar to early stage metabolic dysfunction discussed in our blog “Insulin Resistance: The Silent Phase Before Type 2 Diabetes”. Fertility disruption often begins years before diabetes risk becomes visible.
Inflammation originating from gut dysbiosis or excess visceral fat further amplifies ovarian stress. The ovaries are highly sensitive to inflammatory cytokines.
Micronutrient deficiencies such as magnesium, zinc, selenium, vitamin D, and B vitamins impair hormone synthesis and detoxification pathways.
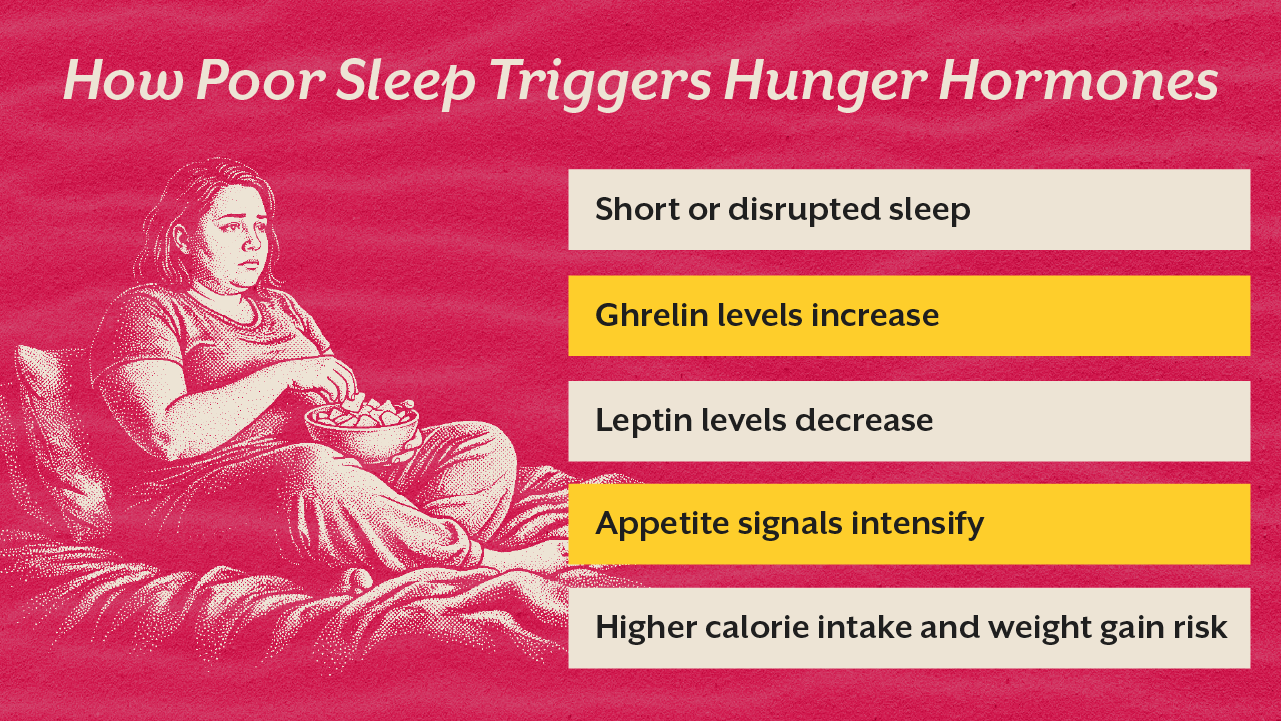
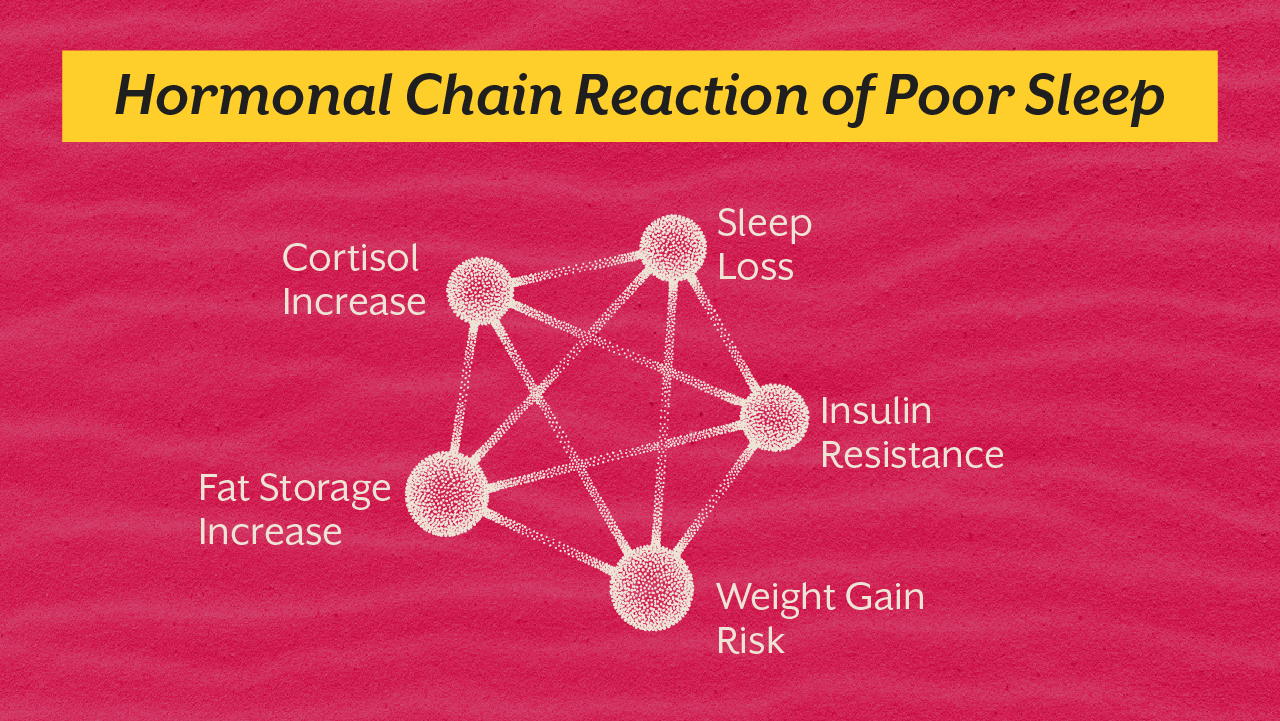
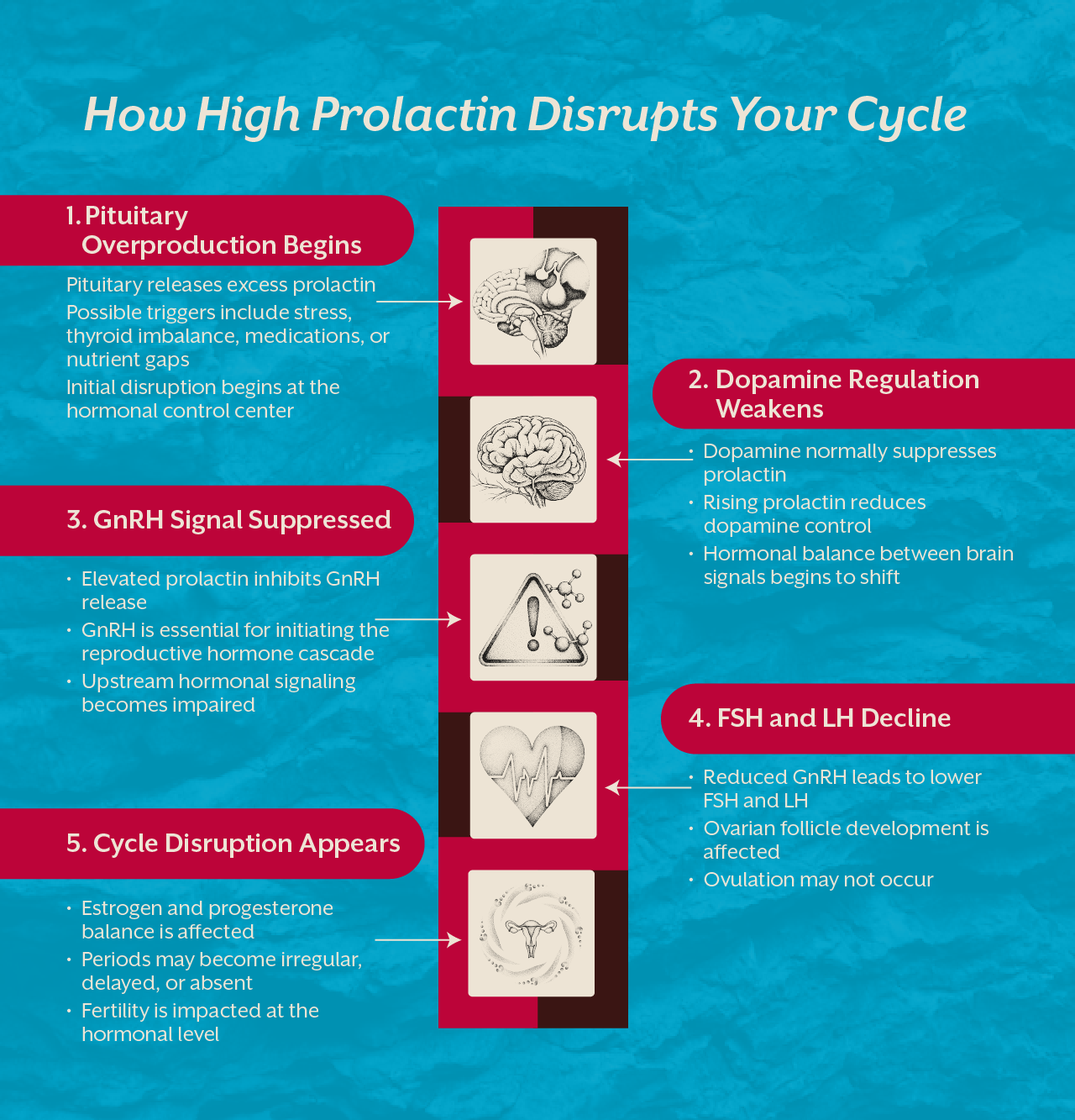
Sleep disruption and chronic stress increase cortisol, which alters GnRH pulsatility from the hypothalamus. Ovulation depends on precise hormonal timing. Chronic stress scrambles that rhythm.
When women ask about the best treatment for PCOS to get pregnant, the answer lies in restoring metabolic flexibility, improving insulin sensitivity, reducing inflammation, and supporting cellular energy.

Rethinking PCOS Fertility Treatment
Many women are prescribed ovulation induction medications. While these may stimulate ovulation, they do not correct underlying metabolic dysfunction. Without addressing insulin resistance and inflammation, conception may remain difficult or early miscarriage risk may increase.
At iThrive Alive, the approach begins with root cause evaluation. Fasting insulin, HOMA IR, inflammatory markers, nutrient panels, thyroid optimization, and gut health assessment help identify drivers.
Lifestyle intervention is foundational. Smart eating types that stabilize blood glucose, structured resistance training to improve insulin sensitivity, circadian aligned sleep, and nervous system regulation are non-negotiable pillars.
Targeted supplementation supports cellular repair. In specific cases, inositol for insulin signaling, omega-3 fatty acids for inflammation control, magnesium for glucose metabolism, and antioxidant support for mitochondrial resilience are integrated.
We have seen this transformation in our published case study “Targeted Nutritional Intervention in PCOS-Associated Metabolic Dysfunction: A Root Cause Analysis & Functional Nutrition driven Case Study”. When metabolic markers improved, menstrual cycles regularized and ovulation resumed naturally.

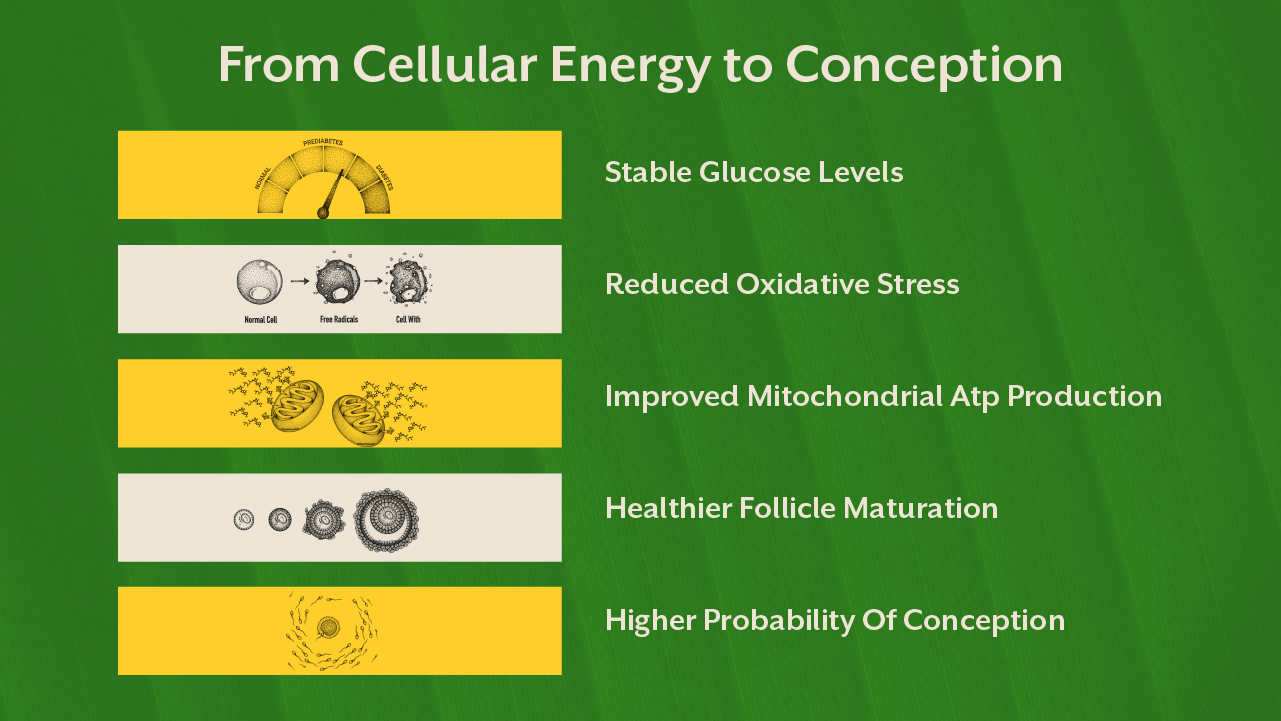
Egg Quality and Mitochondrial Health
PCOS pregnancy success is not just about ovulation frequency. Egg quality matters profoundly. Mitochondria within the oocyte determine energy supply for fertilization and early embryo development.
Oxidative stress damages mitochondrial DNA. High glucose fluctuations increase free radical production. Micronutrient insufficiency reduces antioxidant defense systems.
Nutrients such as CoQ10, magnesium, B vitamins, and omega-3 fatty acids support mitochondrial efficiency. However, supplementation without dietary correction rarely produces sustainable change.
When women feel frustrated that cycles are irregular or that fertility treatments have failed, it is important to understand that improving cellular energy is a gradual biological process. Internal repair precedes visible reproductive change.
A Systems Approach to PCOS Pregnancy
Polycystic ovary syndrome is not a barrier sentence. It is a signal. A signal that metabolic systems require attention.
When gut integrity improves, inflammation reduces. When insulin sensitivity improves, androgen excess declines. When mitochondria function efficiently, egg quality improves. When stress physiology stabilizes, ovulatory rhythm normalizes.
This is why we emphasize evaluation beyond basic hormone panels. Through a structured root cause analysis, women gain clarity about why ovulation is irregular and what is blocking conception. For those seeking guidance, you can book a root cause analysis or book a consult to understand your unique metabolic drivers.
PCOS fertility treatment is most effective when it restores biological intelligence rather than overriding it.
What You Can Do If You Want to Improve PCOS Pregnancy Outcomes
If pregnancy is your goal, the sequence in which you repair physiology matters. Ovulation is the last domino. Metabolic signaling is the first.
1. Lower Fasting Insulin Before You Focus on Ovulation
In PCOS, hyperinsulinemia stimulates ovarian theca cells to overproduce androgens via insulin receptor cross activation of LH signaling pathways. Elevated insulin also suppresses hepatic SHBG production, increasing free testosterone.
What this means practically:
Stabilize postprandial glucose excursions.
Anchor meals around adequate protein.
Avoid frequent grazing that perpetuates insulin spikes.
Incorporate resistance training to enhance GLUT4 translocation in skeletal muscle independent of insulin.
When insulin reduces, androgen excess gradually declines, allowing follicular selection to normalize.
2. Reduce Inflammatory Signaling That Impairs Follicular Maturation
Inflammatory cytokines such as TNF alpha and IL 6 interfere with granulosa cell function and steroidogenesis. Chronic low grade inflammation also worsens insulin resistance in a feedback loop.
Clinically, this means:
Repair gut barrier integrity.
Improve microbial diversity.
Ensure omega-3 sufficiency.
Prioritize sleep because sleep restriction elevates CRP and cortisol.
Reducing inflammatory load improves ovarian microenvironment quality.
3. Replete Micronutrients Required for Hormone Synthesis
Ovarian steroidogenesis is nutrient dependent. Magnesium acts as a cofactor in ATP dependent enzymatic reactions. Zinc supports follicular development. Selenium influences thyroid conversion which indirectly affects ovulatory rhythm. B vitamins support methylation pathways essential for hormone detoxification.
Without micronutrient sufficiency, even pharmacological ovulation induction may yield suboptimal egg quality.
Testing and repletion must be personalized rather than supplemented blindly.
4. Support Mitochondrial Efficiency to Improve Egg Quality
The oocyte contains the highest mitochondrial density of any cell in the female body. Mitochondrial dysfunction reduces ATP availability required for meiotic spindle formation and embryo development.
Interventions include:
Improving glycemic variability.
Correcting oxidative stress.
Targeted antioxidants such as CoQ10 where clinically indicated.
Strength training to improve systemic mitochondrial biogenesis.
Circadian alignment to enhance cellular repair cycles.
Egg quality restoration is gradual because folliculogenesis spans several months.
5. Regulate Stress Physiology to Normalize GnRH Pulsatility
Chronic sympathetic dominance alters hypothalamic GnRH pulse frequency. This disrupts LH and FSH balance, further impairing ovulation.
Nervous system regulation, breath work, light exposure, consistent sleep timing, and emotional stress processing are not secondary. They directly influence reproductive hormone rhythm.
6. Test Before You Escalate
Before proceeding to aggressive assisted fertility protocols, evaluate:
- Fasting insulin
- HOMA IR
- Inflammatory markers
- Thyroid conversion
- Vitamin D
- Iron status
- Androgen levels
- Gut health where indicated
This is where a structured root cause analysis becomes valuable. It prevents guesswork and reduces unnecessary hormonal exposure.
For women who want clarity instead of assumptions, you can book a root cause analysis or book a consult to understand which layer of dysfunction is most relevant in your case.
Key Takeaway
If you are navigating PCOS and longing for pregnancy, understand that your body is not broken. It is responding to metabolic signals that can be influenced. Ovulation is a reflection of systemic health. By addressing insulin resistance, inflammation, mitochondrial dysfunction, and lifestyle rhythms, fertility potential improves organically. The best treatment for PCOS to get pregnant is not a single pill or protocol. It is a coordinated restoration of metabolic balance that allows the ovaries to function as they were designed to.